
Introduction
Healthcare organizations face a persistent challenge: wide variation in provider performance remains common and often unmeasured, particularly in rural settings. A 2022 cross-sectional study documented sizeable physician-level practice variations across common clinical scenarios, even among physicians treating similar patients.
This inconsistency affects patient outcomes, drives unnecessary costs, and makes equitable care harder to deliver.
The gap exists partly because many healthcare systems lack the infrastructure to systematically measure performance. Administrative capacity constraints, fragmented data systems, and limited technical staff make robust profiling challenging for rural organizations. Addressing this variation is essential for improving care quality and supporting strategic workforce decisions around provider retention and recruitment.
Provider profiling is one practical response to that challenge — a data-driven process for measuring clinical quality, resource use, and patient experience across providers. This guide covers what profiling is, its guiding principles, how it works in practice, and what best practices look like for rural healthcare organizations building credible programs.
Key Takeaways
- Provider profiling systematically measures healthcare provider performance using clinical quality, resource use, and patient satisfaction data.
- Effective programs require clinically grounded measures, adequate risk adjustment, physician involvement, and standardized data collection.
- Performance measures fall into four categories: clinical outcomes, process of care, patient perceptions, and resource use.
- Small sample sizes, poor data quality, and low physician buy-in can be resolved through reliable data infrastructure and early physician involvement.
- For rural organizations, establishing a reliable data foundation is the critical first step toward meaningful profiling.
What Is Provider Profiling in Healthcare?
Provider profiling is the systematic effort to measure the performance of individual physicians, NPs, PAs, or practice groups by analyzing patterns in clinical quality, resource use, and patient experience data. According to a 2003 BMJ article, profiling gives interested parties insight into the structure, process, and outcomes of care delivery. The terms "physician profiling," "provider profiling," and "performance profiling" are used interchangeably.
Two primary types of profiling exist:
- Clinical profiling examines practice patterns and outcomes—what care is delivered and what results it achieves
- Economic profiling examines financial patterns and cost efficiency of a provider's practice
Effective programs integrate both dimensions — clinical and economic — to give decision-makers a full view of provider performance.
Key stakeholders use profiling data for distinct purposes:
| Stakeholder | Purpose |
|---|---|
| Health Systems | Guide quality improvement and workforce planning |
| Payers | Assess value and manage networks |
| Accrediting Bodies | Verify compliance and accreditation standards |
| Patients | Make informed provider choices |

How these stakeholder interests are balanced directly shapes program design. Systems oriented primarily toward cost control tend to generate physician resistance, while those emphasizing quality improvement see better engagement and outcomes.
Profiling vs. Credentialing: Understanding the Distinction
Provider profiling focuses on ongoing performance measurement—how well a provider practices over time. Credentialing verifies qualifications, licensure, and eligibility to practice at a point in time. Both are necessary for comprehensive provider management, but they serve different functions and should not be treated as interchangeable in program design. In practical terms: credentialing asks "Is this provider qualified?" while profiling asks "How is this provider performing?"
The Core Principles That Guide Effective Provider Profiling
Primary goal is quality improvement, not punishment
The foundational purpose of profiling should be to give providers meaningful, actionable feedback that helps them improve care. Research documents that purchasers have largely developed physician profiling as a tool to control costs rather than measure and improve quality. This approach generates physician skepticism and resistance. Programs designed around improvement rather than accountability consistently achieve better engagement and outcomes.
Releasing data alone changes little. Profiling must be paired with structured support to help providers actually change how they deliver care. A 2003 BMJ study found that punitive profiling programs can push physicians to avoid sicker patients — an outcome that harms the populations these systems are meant to protect.
Physician involvement is non-negotiable
Providers must participate in developing performance measures and profiling methods—not merely receive reports. When physicians lack ownership of the process, they are often unaware of or uninfluenced by profiling results. A 2005 Commonwealth Fund report found only one-third of physicians had any comparative performance data available to them.
Meaningful physician involvement includes:
- Participating in measure selection and validation
- Reviewing and commenting on draft reports before release
- Helping interpret results and identify improvement opportunities
- Co-designing feedback mechanisms and improvement interventions
Performance measures must be clinically relevant and scientifically grounded
Strong measures share four characteristics: high prevalence in the practice population, clear links to patient outcomes, an evidence base from randomized trials or structured consensus, and direct actionability by the provider being measured. The NQF consensus development process evaluates measures against five criteria, with scientific acceptability — covering validity and reliability — as a must-pass standard.
Endorsement status alone isn't sufficient vetting. A 2023 review found that most NQF standing committee members voted moderate rather than high support on key assessment criteria, even though 91.56% of reviewed measures ultimately received endorsement. Organizations should examine the underlying validity evidence directly.
Physician involvement in measure selection (covered above) directly reinforces this principle — clinicians are best positioned to identify whether a measure reflects what actually happens in practice.
Accountability must be limited to what the provider actually controls
Accurate attribution is essential—a physician should only be evaluated on patients and services for which they are directly responsible. Episode-based profiling assigns responsibility to physicians who account for a defined threshold (typically 30% or more) of professional and prescribing costs within an episode.
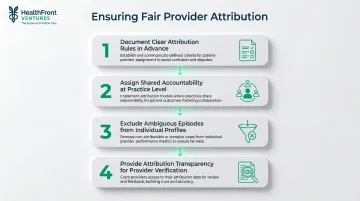
Shared care arrangements, multidisciplinary teams, and cross-coverage complicate attribution. Solutions include:
- Using clear attribution rules documented in advance
- Assigning shared accountability at the practice level rather than individual level
- Excluding episodes with ambiguous attribution from individual profiles
- Providing attribution transparency so providers can verify which patients are included
Standardization and minimal duplication
Use consistent core performance measures across payers and settings to reduce redundant reporting burden. A 2009 HSChange report documented that different plans may use different measures or measure the same thing differently—a physician can be simultaneously rated as a high performer by one plan and a low performer by another. Because any single plan's patients represent only a small fraction of a physician's panel, inconsistent measurement produces incomplete and misleading assessments.
Multi-payer data aggregation and standardized measure sets are prerequisites for credible profiling.
Types of Performance Measures Used in Provider Profiling
Clinical Outcomes
Clinical outcome measures include mortality rates, non-fatal complications, intermediate physiological outcomes such as blood pressure or HbA1c control, symptom relief, and functional capacity. These are the most direct indicators of care quality — and the hardest to dismiss.
Advantages:
- Strongest signal of provider performance
- Most relevant to patient welfare
- Difficult to "game" or manipulate
Limitations:
- Require robust risk adjustment for fair comparison
- More expensive to collect than administrative data
- Affected by factors beyond provider control
- Small sample sizes limit statistical reliability
AHRQ cautions that outcome data reflects far more than provider behavior alone — patient demographics, comorbidities, and social factors all shape results. Until risk-adjustment methods catch up, outcome measures can mislead as easily as they illuminate.
Process of Care Measures
Process measures indicate whether evidence-based care steps were taken—appropriate medication prescribing, screening rates, timely access to care, preventive service delivery. AHRQ reports that the majority of healthcare quality measures used for public reporting are process measures.
Process measures are widely used for good reason:
- Easier to collect from administrative data
- Directly actionable for quality improvement
- Less affected by patient case-mix when properly specified
- Provide clear feedback on specific behaviors
One firm requirement: each process measure must have a demonstrated link to patient outcomes. Measuring compliance with outdated or unproven practices wastes resources and erodes the credibility of the entire profiling program.
Patient Perceptions
Patient experience and satisfaction data capture dimensions that only patients can evaluate: symptom relief, continuity of care, quality of communication, respect and dignity, appointment accessibility, and care coordination.
AHRQ's CAHPS Clinician & Group Survey asks patients to report on experiences with providers and staff, covering:
- Accessibility of care
- Communication with providers
- Care coordination
- Interactions with staff
Critical sample size consideration: A 2017 study published in the Journal of General Internal Medicine found that reaching 0.90 reliability at the individual physician level requires approximately 255 completed patient surveys—far exceeding the CAHPS Consortium's standard recommendation of 50. The physician-level effect accounted for only 3.4% of total variance, with patient factors explaining far more.
Implication for rural practices: With small patient panels, patient experience measures should be aggregated to the practice or group level rather than individual provider level to achieve statistical reliability.
Resource Use and Cost Measures
Resource use metrics include utilization rates, cost per episode, length of stay, referral rates, and prescribing patterns. These measures are important for understanding efficiency but carry risk if overemphasized.
Used responsibly, resource measures support efficiency without undermining care quality:
- Pair with quality data to prevent incentivizing undercare
- Use to raise awareness and support efficiency discussions
- Apply transparent risk adjustment to account for patient complexity
- Frame as learning opportunities rather than punitive benchmarks
Episode-based profiling mines claims, pharmacy, laboratory, and administrative data to construct patient episodes and attribute costs based on contribution thresholds. Despite its sophistication, a 2008 analysis found that this approach creates numerous opportunities to misidentify high and low performers — driven by coding variation, attribution errors, and cost outliers.
Data Sources and Risk Adjustment in Provider Profiling
Healthcare organizations draw profiling data from four main sources, each with distinct trade-offs:
| Data Source | Strengths | Limitations |
|---|---|---|
| Medical Records | Clinical depth; detailed patient information | Labor-intensive; not standardized across settings |
| EHR / Clinical Systems | Real-time data; linked lab and pharmacy | Adoption variation; heterogeneous formats |
| Administrative / Claims | Widely available; large samples; standardized codes | Limited clinical depth; coding variability |
| Patient Surveys (CAHPS) | Standardized; captures patient perspective | Requires large samples; costly to administer |
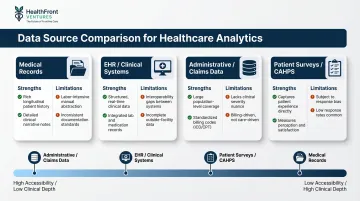
Each source involves trade-offs between accessibility and clinical depth. Linking data types — pharmacy, lab, and claims — increases analytical accuracy but requires meaningful infrastructure investment. That infrastructure gap becomes especially pronounced when accounting for patient complexity, which is where risk adjustment enters the picture.
Risk Adjustment Is Essential
Providers who care for sicker or more complex patients will appear to perform worse without proper risk adjustment. Case-mix adjustment accounts for differences in patient demographics and diagnoses, while disease severity adjustment accounts for the acuity and complicating factors within conditions.
Critical requirements for risk adjustment:
- Documented methodology open to inspection
- Validated against observed outcomes
- Transparent and reproducible (no "black box" algorithms)
- Appropriate to the measure and clinical context
AHRQ notes that risk adjustment methods are still maturing — organizations should treat any single methodology as a starting point, not a final authority, and revisit their approach as better tools emerge.
Rural Data Infrastructure Challenges
Rural healthcare organizations face unique barriers to robust profiling. According to a 2024 HRSA report, over 5,200 Rural Health Clinics serve more than 60% of rural Americans—yet many lack the administrative capacity for quality reporting.
Specific rural obstacles include:
- RHCs cannot use CPT Category II quality codes on Medicare claims without risking rejection of the entire claim
- Same-day billing restrictions limit access to performance data
- Fragmented EHR systems across small practices
- Small patient panels per provider limit statistical reliability
- Limited technical staff to manage data infrastructure
Outsourced data services — like HealthFront Ventures' HCP Workforce Data Warehouses — offer one path forward, handling claims normalization and NPI-level provider data so rural organizations can access analytics-ready datasets without building custom infrastructure from scratch.
Challenges in Provider Profiling and How to Address Them
Small sample sizes and statistical reliability
At the individual provider level, small patient volumes create high measurement error and unreliable performance estimates. AHRQ identifies the difficulty of constructing valid measures with data from small patient populations as a primary technical challenge.
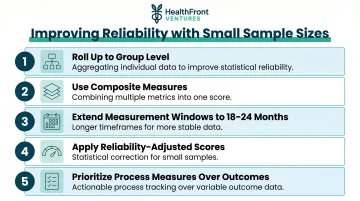
Ways to improve reliability:
- Roll up results to group or practice level
- Use composite measures combining multiple indicators
- Extend measurement windows (e.g., 18–24 months instead of 12)
- Apply reliability-adjusted scores (shrinkage estimators) before making decisions
- Focus on process measures rather than outcomes when volumes are insufficient
A 2009 Health System Change report on physician profiling found that although plans typically require minimum sample sizes, thresholds tend to be set relatively low—fewer than a dozen patients in some cases—yielding incomplete and unreliable information.
Data quality and inconsistent definitions
Coding errors, upcoding, incomplete records, and inconsistent data definitions undermine profiling validity. Physicians who electronically submit accurate, fully documented claims tend to have more reliable episode profiles; those with inconsistent documentation skew comparative results and introduce bias.
Practical steps to address data quality:
- External audits of coding practices
- Standardized data collection protocols
- Centralized data processing to ensure consistency
- Regular validation against chart review samples
- Clear documentation requirements shared with providers
These problems are especially acute in rural settings, where administrative infrastructure is often limited. HRSA's 2024 report documents that Rural Health Clinics (RHCs) lack federal grant support for quality reporting infrastructure—a gap that FQHCs and Critical Access Hospitals don't face.
Physician resistance and lack of trust
Data quality issues don't exist in isolation—they feed directly into physician resistance. Providers who distrust the underlying data are rarely willing to engage with the results. That resistance typically stems from concerns about accuracy, inadequate risk adjustment, and fear that profiles will be used punitively rather than constructively. The American Medical Association's physician-led profiling program ended in 2001 due to cost overruns and questionable variable choices. A similar Maine project collapsed after failing to secure support from professional bodies or purchasers.
How to build physician trust:
- Involve physicians in measure development from the start
- Give providers time to review and comment on reports before release
- Frame results around improvement, not accountability
- Ensure risk adjustment methods are transparent and defensible
- Provide specific, actionable feedback tied to improvement pathways
AHRQ cites physician wariness and lack of consensus about appropriate measures as political challenges in physician measurement programs.
Best Practices for Building a Sound Provider Profiling System
Design reports with clear intent and audience in mind
Distinguish between internal and external profiling reports. Internal reports support quality improvement and peer review, with appropriate confidentiality protections. External reports require higher standards of statistical validity, physician review before release, and distribution on a "need to know" basis.
A 2021 realist review found that bottom-up initiated audits are more likely to bring about sustained change compared to externally imposed audits. However, the review also found that after about three years, the rate of improvements tailed off—highlighting the importance of evolving the profiling program over time.
Quality assurance privilege under state laws shields proceedings and records related to performance review from disclosure, but organizations should document committee processes rather than specific statements to preserve this protection.
Establish a regular reporting cadence tied to improvement goals
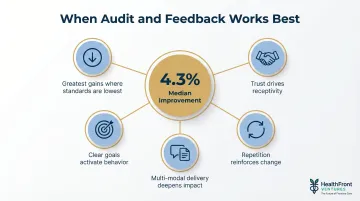
Annual reports may suffice for accreditation comparisons, but quality improvement initiatives require more frequent feedback. The Cochrane review by Ivers et al. analyzed 140 studies and found that audit and feedback generally leads to small but potentially important improvements—a median 4.3% absolute increase in compliance with desired practice.
Feedback is most effective when:
- Baseline performance is low
- The source is a supervisor or colleague
- It is provided more than once
- It is delivered in both verbal and written formats
- It includes explicit targets and an action plan
Rotating supplemental measures alongside core measures keeps the system adaptive, reduces "gaming," and addresses new priorities as they emerge.
Treat profiling as one component of a broader workforce and quality strategy
Releasing data alone accomplishes little—profiling must be followed by structured efforts to act on findings. Rural organizations, in particular, can connect profiling directly to workforce strategy:
- Inform recruitment decisions by identifying specialty and geographic gaps
- Identify retention risks by monitoring provider satisfaction and workload metrics
- Support structured planning around NP/PA workforce development
- Align with performance frameworks that tie quality and access to compensation
HealthFront Baseline™ supports this integration by combining quantitative workforce metrics—supply, distribution, and utilization—with rural county quality measures, giving organizations the data foundation needed to act on profiling findings without building custom reporting infrastructure.
Frequently Asked Questions
What is provider profiling in healthcare?
Provider profiling is the systematic measurement of a healthcare provider's clinical performance, resource use, and patient experience. It's used to improve care quality, ensure accountability, and support informed decision-making by patients, health systems, and payers.
What are the two main types of provider profiling?
Clinical profiling examines practice patterns and outcomes—what care is delivered and what results it achieves. Economic profiling examines cost and resource utilization patterns. Programs that integrate both can connect cost patterns directly to clinical outcomes, making benchmarking far more actionable.
What data sources are used to build provider profiles?
The four primary sources are medical records, electronic health records, administrative and claims data, and patient surveys. Administrative data is widely available but clinically shallow; medical records offer depth but require significant processing effort.
Why is risk adjustment important in provider profiling?
Without risk adjustment, providers caring for sicker or more complex patients appear to perform worse than peers, creating unfair and misleading comparisons. Risk adjustment accounts for differences in patient case-mix and disease severity to enable valid benchmarking.
How can organizations build physician buy-in for profiling programs?
Start by involving physicians in developing the measures and giving them a chance to review reports before release. Framing results around quality improvement—rather than penalties—and ensuring data is accurate and fairly risk-adjusted are what turn skeptics into advocates.
What unique challenges does provider profiling present in rural healthcare settings?
Rural settings face small patient panels per provider (limiting statistical reliability), fragmented or absent integrated data systems, limited technical infrastructure, and structural exclusion from federal programs like MIPS. Purpose-built rural HCP data solutions with outsourced infrastructure are helping address these gaps.