
The timing is critical. Between 2005 and 2023, 146 rural hospitals closed or stopped providing inpatient services, leaving entire communities without local emergency care. 63.1% of primary care health professional shortage areas are in rural counties, and 15,628 additional primary care physicians are needed to close the gap nationwide. Rural residents face higher mortality rates from heart disease, cancer, and chronic respiratory disease compared to urban populations, with maternal mortality nearly twice as high in rural areas.
This article explains how the program works, its five strategic pillars, what funding means for rural health organizations, and why workforce data infrastructure is essential for successful execution.
Key Takeaways
- CMS distributes $50 billion over five fiscal years (2026–2030), with $10 billion awarded annually across all 50 states
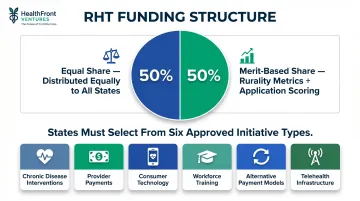
- Half of funding is distributed equally among states; half is awarded based on rurality metrics and proposed initiative impact
- Five strategic pillars guide spending: rural health promotion, sustainable access, workforce development, innovative care models, and technology innovation
- CMS created the Office of Rural Health Transformation to oversee implementation and provide each state with dedicated project officers
- CMS reporting standards require states to submit quantitative workforce outcome data — rural organizations without baseline metrics risk falling short at review
The Rural Health Crisis That Made This Investment Necessary
Over 60 million Americans—roughly one in five—live in rural areas, yet these communities face the most severe healthcare access challenges in the nation. More than 35% of U.S. counties are maternity care deserts, with nearly two-thirds of those deserts located in rural areas, leaving pregnant women hours away from obstetric services. In 2023, 7.2% of U.S. counties had no primary care physician at all.
The workforce shortage compounds these access gaps. Rural communities face higher provider vacancy rates, weaker recruitment pipelines, and limited retention incentives compared to urban markets.
The scale of the shortage is hard to overstate: 8,466 designated primary care health professional shortage areas exist nationwide, 63.1% of them in rural areas. Closing those gaps would require over 15,000 additional primary care physicians.
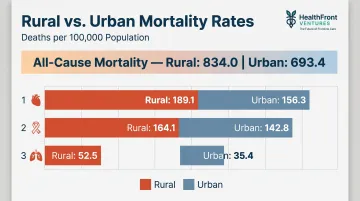
These access barriers translate directly into worse health outcomes. Rural residents experienced age-adjusted all-cause mortality rates of 834.0 per 100,000 in 2019, compared to 693.4 in urban areas. Rural populations die at higher rates from:
- Heart disease: 189.1 vs. 156.3 per 100,000 (urban)
- Cancer: 164.1 vs. 142.8 per 100,000
- Chronic lower respiratory disease: 52.5 vs. 35.4 per 100,000
Rural hospital closures have also significantly increased EMS transport and activation times, delaying emergency care when minutes matter most.
The federal response came through Section 71401 of the Working Families Tax Cuts Act (Public Law 119-21), commonly called the One Big Beautiful Bill Act. It established the $50 billion Rural Health Transformation Program—the largest single federal investment in rural health infrastructure to date—directing states to build the workforce and delivery systems these communities have lacked for decades.
How the $50 Billion RHT Program Works
CMS structured the RHT Program as a five-year initiative running from federal fiscal year 2026 through 2030, distributing $10 billion annually. First-year awards were announced December 29, 2025, with states moving immediately into implementation planning.
Funding Formula
The allocation uses a 50/50 split designed to balance baseline support with merit-based incentives:
- Equal share (50%): Distributed among all approved states, providing a foundation regardless of size or population
- Merit-based share (50%): Allocated by rurality metrics, proposed policy actions that improve rural access and quality, and application scoring for measurable impact potential
Every rural state receives a meaningful baseline — and states with strong execution plans earn more.
Application and Review
All 50 states applied by the November 5, 2025 deadline. CMS evaluated applications through a structured merit review framework using subject matter experts, and all 50 states received approval — a 100% award rate that reflects the program's design as universal infrastructure investment, not a competitive grant.
Program Governance
CMS provides ongoing support and accountability through several mechanisms:
- Project officers: Dedicated to each state for technical assistance and day-to-day coordination
- Progress reporting: States submit regular updates to track implementation milestones and outcomes
- Annual Rural Health Summit: States convene to share lessons and accelerate cross-state learning — the inaugural Summit ran alongside the 2026 CMS Quality Conference
Compliance Requirements
Governance sets the oversight structure — but states also face specific funding conditions. Each must direct resources toward at least three approved initiative types, which can include:
- Evidence-based chronic disease interventions
- Provider payments for specified services
- Consumer-facing technology solutions
- Workforce training and recruitment programs
- Alternative payment model development
- Telehealth and remote patient monitoring infrastructure
This flexibility allows states to tailor investments to local rural health priorities while maintaining federal accountability standards.
The Five Strategic Pillars of the RHT Program
The program organizes funding around five strategic pillars that address the full spectrum of rural health challenges.
Pillar 1: Make Rural America Healthy Again
This pillar funds preventive care expansion, chronic disease management, maternal health services, and behavioral health programs. States can invest in evidence-based interventions including:
- Food-as-medicine programs addressing nutrition-related chronic conditions
- Physical fitness and wellness initiatives targeting root causes of poor health outcomes
- Prenatal and postnatal care access improvements
- Mental health and substance use disorder treatment infrastructure
The focus is upstream: preventing disease and managing chronic conditions before they require expensive emergency interventions.
Pillar 2: Sustainable Access
Keeping rural healthcare access points viable long-term requires operational innovation. This pillar supports:
- Care coordination and hub-and-spoke delivery models
- Rural regional centers of excellence that anchor specialty services
- Shared operations and efficiency improvements
- Integrated primary care and specialty care networks
- Emergency medical services coordination
The goal is financial and operational sustainability—ensuring rural providers remain accessible community health anchors.
Pillar 3: Workforce Development
The workforce crisis sits at the heart of rural health transformation. This pillar funds clinical training programs, residency pathways, and recruitment and retention incentives for healthcare providers.
CMS requires participating organizations to report quantitative workforce metrics throughout the five-year program period—MD and NP/PA retention rates, vacancy rates, and rural county quality measures. Organizations that build data infrastructure early are better positioned to demonstrate progress and protect their funding allocations.
Pillar 4: Innovative Care Models
This pillar accelerates the shift toward value-based care and payment innovation:
- Alternative payment mechanisms and risk-sharing arrangements
- Accountable care organizations and clinically integrated networks
- Telehealth infrastructure and remote patient monitoring
- Advanced primary care medical home models
These models tie payment to patient outcomes rather than visit volume—a structural shift that rural providers have long needed to make preventive care financially viable.
Pillar 5: Technology Innovation
Rural providers face unique technology challenges, from cybersecurity vulnerabilities to interoperability gaps. This pillar invests in:
- Cybersecurity infrastructure to protect patient data
- Interoperability solutions enabling seamless data sharing across providers
- AI-assisted clinical workflow tools, including AI scribes that reduce documentation burden
- Digital health tools for both providers and patients
For many rural organizations running on legacy systems, this funding offers a direct path to closing the technology gap with urban health systems—without building from scratch.

State Award Breakdown: Who Gets What and Why
First-year awards range from $147 million (New Jersey) to $281 million (Texas), with a national average of approximately $200 million per state. This range reflects the rurality and impact-potential components of the 50/50 allocation formula.
Notable State Examples
Texas ($281 million): Technology infrastructure, clinically integrated networks, and provider payments anchor this award — the largest in the nation — spanning the state's vast rural geography.
Alaska ($272 million): Primary care access and obstetric services take center stage, directly addressing the isolation challenges facing rural communities spread across a state larger than most countries.
Montana ($234 million): Workforce development leads here, with funding targeting provider recruitment and retention alongside keeping rural hospitals financially viable.
Universal Participation
All 50 states received awards — a 100% approval rate that confirms this is a universal infrastructure program, not a competitive grant. That distinction matters for planning: every state already has a funded transformation plan in motion, which means state-level workforce and data programs can align execution now rather than wait on award outcomes.
Key implications for state stakeholders:
- No states were excluded, removing the uncertainty that typically delays program planning
- Funded plans are active in all 50 states, enabling immediate cross-state coordination
- Workforce data infrastructure investments can be timed to align with existing state RHT timelines
What This Means for Rural Healthcare Organizations
The RHT Program creates a five-year funding window for rural health organizations to align workforce expansion, care delivery innovation, and infrastructure modernization plans with state transformation priorities. Proactive engagement with your state's RHT project officer — and alignment to state plan objectives — is what separates organizations that capture funding from those that watch it pass by.
The Measurement Imperative
CMS requires states to submit regular progress updates and track program outcomes. Rural health organizations lacking baseline data infrastructure will struggle to demonstrate impact and sustain funding. Quantifiable workforce metrics—provider retention rates, NP/PA vacancy rates, rural county quality measures—are essential contributions to state reporting requirements.
HealthFront Baseline™ addresses this directly. The service provides FY25 baseline data metrics across four quantitative workforce measures plus one rural county quality measure, delivered through an AI-native data warehouse built specifically for rural HCP workforce reporting. Organizations can feed these metrics directly into state RHT progress submissions without building custom data infrastructure.
Act Now
With FY26 funds already in motion, states are in active implementation planning. Rural healthcare organizations, community health centers, and workforce programs should align their data collection, workforce planning, and partnership structures to state RHT goals without delay. The five-year program clock is already running — organizations without baseline data in place cannot retroactively establish a starting point.
Key action steps:
- Contact your state's RHT project officer to understand state plan priorities
- Identify which of the five strategic pillars align with your organization's strengths
- Establish baseline workforce and quality metrics to track progress
- Consider data infrastructure that enables ongoing measurement and reporting
- Build partnerships with other rural providers to share resources and capabilities

Frequently Asked Questions
How many states applied for the rural health transformation fund?
All 50 states applied by the November 5, 2025 deadline, and all 50 were approved as awardees. Unlike competitive grant programs, the RHT Program funds every state — making it a universal federal investment in rural health infrastructure.
What does the Big Beautiful Bill do for rural hospitals?
The $50 billion RHT Program was established by the One Big Beautiful Bill Act (Public Law 119-21) to fund rural hospital sustainability, workforce development, technology modernization, and innovative care models across five fiscal years (2026–2030).
What does CMS consider rural?
CMS defines rural areas using criteria from the RHT Program NOFO and Public Law 119-21. In practice, this includes non-metropolitan statistical area designations and county-level rurality indicators used across federal rural health programs.
What percentage of Medicaid goes to rural areas?
24% of rural residents have Medicaid coverage compared to 21% of urban residents, making Medicaid the second-largest coverage source in rural areas. Nearly half of rural births are covered by Medicaid, underscoring rural communities' disproportionate dependence on the program.
What is the Office of Rural Health Transformation (ORHT)?
Established within CMS's Center for Medicaid and CHIP Services on December 29, 2025, the ORHT is led by Director Alina Czekai. The office oversees RHT Program implementation, provides technical assistance to states, and maintains accountability through the program's end date of September 30, 2031.
How are RHT Program funds distributed among states?
CMS uses a 50/50 allocation formula: half is split equally among all approved states to provide a baseline foundation, while the other half is distributed based on rurality metrics, state policy commitments enhancing rural access and quality, and application quality scored for potential impact on rural community health outcomes.


