Introduction
Rural Kansas faces a healthcare access crisis. 32% of rural hospitals in Kansas are at immediate risk of closure — the highest percentage nationally — and of the state's 107 rural hospitals, 31 are classified as vulnerable.
Provider shortages compound the pressure: many rural counties lack sufficient primary care physicians, mental health providers, and specialists. With 34% of adults age 65 and older living in rural areas, coordinated federal intervention is overdue.
The Rural Health Transformation Program (RHTP) is the federal response: a $50 billion, five-year commitment authorized by Congress and administered by CMS. Kansas secured one of the largest state awards nationally — $221.9 million for year one — funding concrete improvements in care access, provider recruitment, and local health system sustainability.
This blog covers how the program works, what grant opportunities are open to Kansas providers right now, and what the state's five RHTP initiatives mean for rural communities across Kansas.
TLDR: Key Takeaways
- RHTP is a $50 billion federal program; Kansas received $221.89 million for year one
- Funding splits into baseline (equal distribution) and workload (competitive, performance-based)
- Two Kansas grant programs are open now: Regional Partnership Grant ($44M) and REH Conversion/Capital Investment ($15M)
- Kansas's five initiatives target preventive health, provider efficiency, workforce retention, innovative care models, and technology access
- Future funding depends on documented progress against measurable milestones
What Is the Kansas Rural Health Transformation Program?
The Rural Health Transformation Program was authorized by Congress in H.R. 1 (Public Law 119-21) and signed into law on July 4, 2025. The program was created to help state governments support rural communities in improving healthcare access, quality, and outcomes by transforming the delivery ecosystem.
CMS's Five Strategic Goals
CMS established five strategic goals that guide how states design their programs:
- Make Rural America Healthy Again — Focus on prevention and addressing root causes of chronic disease
- Sustainable Access — Strengthen rural provider financial stability and operational capacity
- Workforce Development — Recruit and retain qualified healthcare professionals in rural areas
- Innovative Care — Enable new care delivery models including telehealth and value-based payment
- Technology Innovation — Modernize infrastructure, expand telehealth, and improve cybersecurity

Kansas's application targets Workforce Development, Sustainable Access, and Innovative Care — three of the statute's priority areas — shaping how its governance structure is built to deliver on each.
Kansas's Governance Structure
Kansas Department of Health and Environment (KDHE) serves as the lead state agency, with the University of Kansas Health System Care Collaborative supporting both application development and ongoing grant administration.
To keep funded initiatives grounded in community need, the Governor established the Kansas Rural Health Innovation Alliance (KRHIA). This advisory body provides stakeholder input and oversight throughout the program's execution.
How RHTP Funding Works — Baseline, Workload, and Kansas's $221M Award
RHTP distributes $10 billion annually across five federal fiscal years (FY2026–FY2030). Half ($5B/year) is baseline funding distributed equally to all approved states. The other half ($5B/year) is workload funding distributed competitively.
Three Components of Workload Scoring
CMS uses a three-part technical scoring system to determine competitive workload funding:
- Data-Driven Factors — Based on rural facility counts and population data fixed at submission
- Initiative-Based Factors — Scored on CMS's assessment of quality and execution; states start at 50% credit and increase as milestones are met
- State Policy Actions — Points earned for existing policies and commitments to enact new ones by set deadlines

The Critical "Scoring Ceiling" Concept
A state's initiative-based funding ceiling is fixed at the time of application submission. New initiatives added later do not raise this ceiling, making the initial application's scope the permanent ceiling for initiative-based funding. Year 1 caps states at 50% of their Full Score Potential for initiative-based factors, with additional points available in later years based on documented progress.
Kansas's First-Year Award
That scoring structure directly shaped what Kansas earned. Kansas received $221,898,008 — above the $200M baseline — following CMS's final budget approval on February 17, 2026. States must spend those funds by the close of the following fiscal year.
Annual Re-Scoring
While rural factor data scores remain fixed, initiative-based and policy action scores are reassessed each year based on performance. Future workload allocations are competitive — states that demonstrate measurable progress across three dimensions earn higher shares each year:
- Workforce recruitment and retention
- Rural access improvements
- Quality and outcomes gains
Kansas RHTP Grant Opportunities Available Now
KDHE launched two initial grant programs in February 2026 as the first formal mechanism for Kansas providers to access RHTP funds. Both are administered in partnership with the University of Kansas Health System Care Collaborative.
Regional Partnership Grant Program (RPGP)
Total available: $44 million Application deadline: April 3, 2026
The RPGP funds collaborative arrangements among eligible providers. Grant funds support:
- Preventive healthcare and addressing root causes of disease
- Provider efficiency and sustainability
- Workforce attraction and retention
- Value-based care growth
- Care delivery technology adoption
A wide range of Kansas healthcare organizations qualify. Eligible providers include:
- Kansas hospitals
- Physician practices and solo practitioners
- Rural health clinics
- Federally Qualified Health Centers (FQHCs)
- Local health departments
- Native American Sovereign Tribal facilities
- Certified community behavioral health clinics
- Licensed substance-use disorder facilities
- Licensed long-term care facilities located in rural areas
Rural Emergency Hospital (REH) Conversion / Capital Investment Grant
Total available: $15 million Application deadline: March 20, 2026
The second program takes a different focus. The REH/CAP grant funds facility renovations for organizations converting to — or recently converted to — Rural Emergency Hospital status, plus capital investments for other eligible providers transforming care delivery models.
KDHE hosted an applicant webinar on March 6, 2026 to support organizations preparing applications. Visit the Kansas RHTP website for official RFAs, detailed submission requirements, and restriction information.
The Five Kansas RHTP Initiatives
Governor Laura Kelly outlined Kansas's five RHTP priorities in November 2025, aligning state resources with CMS's strategic goals.
Initiative 1 — Population Health and Preventive Care
This initiative focuses on implementing and sustaining programs that promote preventive healthcare and address root causes of diseases. It connects to CMS's chronic disease management priority area and emphasizes early intervention, health education, and community-based prevention programs.
Initiative 2 — Provider Efficiency and Sustainability
Kansas aims to enhance rural healthcare providers' operational and financial sustainability. RHTP emphasizes provider payment reform and building models resilient beyond FY2030, ensuring local hospitals and clinics can continue serving their communities regardless of shifting federal funding levels.
Initiative 3 — Workforce Recruitment and Retention
Workforce recruitment covers a broad range of allowable investments, including:
- Career pathway programs
- Community health workers (CHWs)
- Doulas and peer support specialists
- Health navigators
K-State Extension will deploy 30 new Extension professionals — including 20 CHWs — in year one, with 20 CHWs employed annually across the full five-year program.
Initiative 4 — Innovative Care Models
Kansas is funding a shift toward value-based care and alternative delivery models, including:
- Community paramedicine for EMS providers
- Telehealth expansion
- Remote patient monitoring
- Specialty care access for rural populations
Together, these models reduce reliance on emergency visits by embedding care coordination into everyday rural health delivery.
Initiative 5 — Technology Innovation
Kansas is investing in consumer-facing technologies including AI-enabled tools, patient apps, wearables, RPM equipment, and data infrastructure upgrades. Kansas is specifically investing in expanded remote patient monitoring and patient-facing AI-enabled health technologies, making digital health infrastructure a funded priority under RHTP for the first time.
Funding Rules, Restrictions, and Compliance
Before applying or planning initiatives, providers must understand consequential spending restrictions:
Spending Caps:
- Administrative expenses: 10% maximum per budget period
- Capital expenditures and infrastructure: 20% maximum
- EHR replacement: 5% maximum
- Startup initiative funding: lesser of 10% or $20M
- Federal salary rate limitations apply to all funded positions
Prohibitions:
- New construction
- Clinical services already reimbursable by insurance
- Urban telehealth specialist payments for rural patients
- Backfilling programs that lost other funding
CMS's Compliance Framework
All funds must align with the approved plan and be expended before the end of the fiscal year following receipt. CMS flags four core non-compliance categories:
- Using funds inconsistently with the approved application
- Failing to enact committed state policy actions
- Inadequate rural investment relative to plan commitments
- Improper fund management or documentation
CMS may withhold, reduce, or recover funds if states fail to correct identified issues.
Reporting Milestones
These compliance expectations feed directly into reporting obligations. States must submit an annual report and funding request for the second budget period by late August 2026. Future funding hinges on satisfactory workplan progress — meaning states that build documentation and performance tracking systems early are far better positioned when renewal decisions are made.
Measuring Workforce Impact to Maximize RHTP Scores
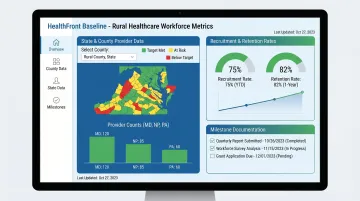
RHTP's competitive workload scoring rewards states and partner organizations that demonstrate measurable, milestone-based progress. Workforce development is one of the key initiative-based technical score factors CMS evaluates. Rural healthcare organizations participating in Kansas RHTP initiatives need structured, data-driven methods to track provider workforce metrics — including physician, NP, and PA recruitment and retention rates — to substantiate progress reports submitted to CMS and KRHIA.
Without a baseline, organizations cannot demonstrate improvement across program years. Building custom workforce tracking infrastructure requires significant investment in data science capacity, systems development, and integration with claims data sources — capacity most rural providers simply don't have.
HealthFront Ventures addresses this directly. Its AI-Native HCP Workforce Data solution provides outsourced data infrastructure — no custom build required. HealthFront Baseline™, launching Q1 2026, delivers FY25 baseline data metrics across 4 quantitative workforce measures plus 1 rural county quality measure, giving organizations the documented starting point CMS requires for credible performance reporting and scoring advancement.
The analytics-ready datasets cover rural healthcare providers at both county and state levels, enabling organizations to:
- Track MD, NP, and PA recruitment and retention rates over program years
- Document progress against CMS milestones with audit-ready data
- Report workforce outcomes without building proprietary systems from scratch
Frequently Asked Questions
Who is eligible to apply for Kansas RHTP grants?
Eligible applicants are Kansas-based rural providers, including hospitals, physician practices, rural health clinics, FQHCs, local health departments, behavioral health and substance-use disorder facilities, long-term care facilities, and Native American Sovereign Tribal facilities.
How much funding did Kansas receive from the Rural Health Transformation Program?
Kansas was awarded $221,898,008 for the first budget period (December 2025 – October 2026), exceeding the $200M baseline and ranking among the top-funded states in the $50 billion national program.
What is the difference between baseline and workload funding in the RHTP?
CMS divides baseline funding equally among all states with approved applications. Workload funding is competitive — CMS scores each state on rural factors data, initiative performance, and policy action commitments to determine its share.
What can Kansas RHTP funds not be used for?
Restrictions include no new construction, no clinical services already reimbursable by insurance, no EHR replacement beyond 5% of funds, no urban telehealth specialist payments for rural patients, and no backfilling programs that lost other funding.
What is the Rural Emergency Hospital (REH) Conversion Grant?
It is a $15M grant available to Kansas facilities converting to REH status for renovations, and to other eligible providers for capital investments that transform how they serve rural communities. The application deadline is March 20, 2026.
How does Kansas track and report progress under the RHTP?
KDHE submits an annual report and funding request to CMS by late August each year. CMS then re-scores workload funding based on initiative milestones met and policy actions implemented — so consistent data tracking directly affects future award amounts.