Key Takeaways
- AI-powered data infrastructure eliminates costly custom builds, bringing enterprise-grade tools within reach of smaller rural facilities
- Federal interoperability rules (FHIR-compliant APIs) became enforceable January 1, 2026—rural systems must now connect or fall out of compliance
- Tracking MDs, NPs, and PAs through recruitment and retention is now a recognized standalone data priority for rural health programs
- Standardized baseline metrics give state RHT programs and rural facilities a shared framework for consistent workforce tracking
The Provider Data Crisis in Rural Healthcare — and Why 2026 Is Different
Rural provider data has historically lived in silos: credentialing records in one system, scheduling in another, EHR documentation in a third, and grant tracking spreadsheets maintained separately.
This fragmentation leaves workforce planners blind to real-time vacancy trends, recruitment teams working from outdated rosters, and retention programs operating without measurable signals. Three forces converged in 2026 to break this pattern.
Federal RHT Funding at Scale
CMS announced $50 billion in Rural Health Transformation awards across all 50 states in December 2025. Texas alone received $1.4 billion over five years—approximately $281 million annually from FY 2026 through 2030. New Jersey and Tennessee launched formal RHT programs with defined workforce incentive activities and quarterly reporting requirements.
Enforceable Interoperability Mandates
The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) required impacted payers to implement Patient Access, Provider Access, Payer-to-Payer, and Prior Authorization APIs by January 1, 2026. While the rule targets payers directly, rural hospitals and critical access facilities face indirect pressure through mandatory payer-provider data exchange.
The Workforce Crisis Itself
HRSA projects nonmetro primary care adequacy will reach only 61% by 2038, creating a 16,070 FTE physician shortage across rural areas. Family medicine alone will be short 6,660 FTEs (71% adequacy), while internal medicine hits 47% adequacy with a 6,420 FTE gap.
Together, these conditions give rural organizations both the mandate and the funding to build provider data infrastructure that actually reflects their workforce in real time.
AI-Native Data Infrastructure Is Replacing the Custom-Build Era
Rather than retrofitting AI onto legacy databases, AI-native infrastructure builds data warehouses and lakes with AI-first architecture from day one. This enables automated data ingestion, intelligent deduplication, and pattern detection on provider records — without manual intervention.
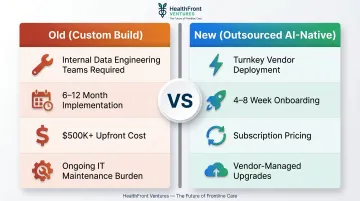
The old model vs. the new:
Old (Custom Build):
- Required internal data engineering teams
- 6-12 month implementation timelines
- $500K+ upfront development costs
- Ongoing maintenance burden on IT staff
New (Outsourced AI-Native):
- Turnkey deployment by third-party vendor
- 4-8 week onboarding windows
- Subscription-based pricing
- Vendor manages upgrades and maintenance
That shift in delivery model unlocks capabilities that custom builds rarely achieved at comparable cost or speed. In 2026, mature AI-native platforms for rural HCP data typically include:
- Automated roster sync across credentialing, HR, and EHR systems to keep provider directories current
- NPI-level matching that reconciles records from disparate platforms without manual cleanup
- Anomaly detection that flags incomplete credentials, missing licenses, or conflicting employment dates
- Predictive analytics that surfaces burnout signals, turnover patterns, and vacancy forecasts
These capabilities also come with compliance infrastructure built in. Modern AI-native HCP platforms integrate HIPAA-aligned encryption, role-based access controls, and audit trails by default — particularly valuable for rural organizations that lack dedicated internal compliance staff.
HealthFront Ventures' AI-Native HCP Workforce Data Warehouses and Lakes are built on this outsourced model, giving rural providers access to the same data infrastructure sophistication as large health systems — without the custom development timeline or upfront cost.
Interoperability Mandates: What Rural Organizations Need to Know
The 2026 Enforcement Landscape
The CMS-0057-F final rule made FHIR-based APIs mandatory for payers starting January 1, 2026. While enforcement targets payers directly, rural health systems must implement compatible infrastructure to exchange data with these newly compliant partners.
On the hospital side, ONC's HTI-1 Final Rule set parallel deadlines:
- By December 31, 2025: Certified health IT modules must support USCDI v3
- APIs must upgrade to HL7 FHIR US Core IG STU 6.1.0 and SMART App Launch 2.0.0
- Service base URLs must publish in standardized FHIR format
The Rural Gap
Most rural hospitals and critical access facilities still operate on HL7 v2 feeds and manual data entry. Moving to FHIR-compliant exchange requires:
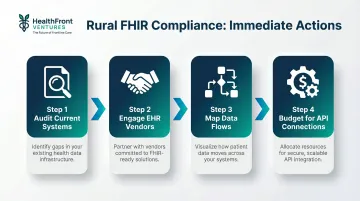
Immediate actions:
- Audit current systems — Identify which platforms support FHIR APIs vs. legacy HL7 v2
- Engage EHR vendors — Confirm USCDI v3 and FHIR US Core IG STU 6.1.0 upgrade timelines
- Map data flows — Document every provider data exchange (payer connections, referral networks, credentialing)
- Budget for API connections — Plan for integration costs if legacy systems require middleware or replacement
The Hidden Opportunity
Working through those four steps does more than satisfy a compliance deadline. FHIR standardization cascades across the entire data environment, improving the quality of records that rural organizations rely on daily for workforce decisions:
- Provider directories stay current as payer connections enforce real-time updates
- Credentialing workflows gain structured data inputs that reduce manual reconciliation
- Cross-system HCP records align across referral networks, reducing duplicate or conflicting entries
- Workforce planning data improves accuracy when the underlying provider data infrastructure is consistent
For rural organizations already stretched thin, that downstream lift in data quality is a concrete operational return—not just a compliance byproduct.
HCP Workforce Data: The Missing Layer in Rural Provider Management
HCP workforce data is distinct from patient or clinical outcomes data. It tracks:
- Provider supply and geographic distribution
- Recruitment pipeline stages and time-to-fill
- Compensation benchmarks by role and region
- Retention signals and turnover patterns
- NP/PA expansion capacity
The Current Gap
Most rural healthcare organizations manage workforce planning through:
- Anecdotal recruitment tracking ("We think we've been hiring slower this year")
- Spreadsheet-based retention monitoring with no trend analysis
- No standardized metrics for benchmarking against peer facilities
- Reactive hiring triggered only after resignations
This makes proactive workforce health management impossible.
What Structured HCP Workforce Data Enables
Structured workforce data shifts rural organizations from reactive to deliberate — across three planning areas:
- Proactive retention: Identify burnout signals — declining patient panel sizes, increased scheduling gaps, reduced CME participation — before resignation letters arrive
- NP/PA expansion: Quantify current MD/NP/PA ratios, geographic coverage gaps, and utilization capacity to build defensible expansion strategies rather than gut-feel hiring
- Incentive program design: Tie retention bonuses, loan forgiveness, and housing assistance to measurable outcomes — years of service, panel growth, quality metrics — that state RHT funders will accept as evidence
The Rural Workforce Reality
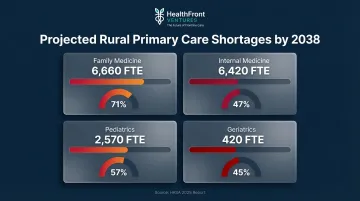
Those capabilities matter more urgently than most rural administrators realize. HRSA's 2025 Primary Care Workforce Report projects severe rural shortages by 2038:
- Family Medicine: 6,660 FTE shortage, 71% adequacy
- Internal Medicine: 6,420 FTE shortage, 47% adequacy
- Pediatrics: 2,570 FTE shortage, 57% adequacy
- Geriatrics: 420 FTE shortage, 45% adequacy
Beyond vacancy numbers, 195 rural hospitals have closed or converted since 2005—110 complete closures and 85 conversions—with workforce gaps cited as a primary contributor.
The Federated Data Model
Rather than building a single centralized workforce database, rural regions are increasingly adopting collaborative models. Individual facilities contribute anonymized workforce data to shared regional pools and draw back aggregate benchmarks and trend insights without surrendering local data control. For state RHT programs, this means actionable regional comparisons — without requiring any single facility to expose its internal numbers.
Standardized Baseline Metrics: The Foundation of Data-Driven Rural Workforce Strategy
Without agreed-upon metrics, rural organizations cannot benchmark performance, demonstrate ROI to state RHT administrators, or satisfy federal grant reporting requirements. When every organization defines "vacancy rate" differently, regional collaboration breaks down.
What a Robust Rural HCP Workforce Baseline Looks Like in 2026
Quantitative metrics:
- Provider vacancy rate by role (MD, NP, PA)
- Average time-to-fill open positions
- Retention duration (median years of service by role)
- Compensation competitiveness vs. regional peers
County-level quality measure:
A geographic access indicator that frames workforce data within rural health realities—accounting for drive time, population density, and HPSA status rather than treating all vacancies equally.
HealthFront Baseline™: The Reference Framework
Launching Q1 2026, HealthFront Baseline™ provides exactly this: 4 quantitative HCP workforce metrics plus 1 Rural County Quality Measure, anchored to FY25 performance data. This gives rural organizations and state RHT programs a standardized starting point for tracking workforce trends going forward.
How Baseline Data Feeds Strategic Planning
With a documented FY25 baseline in place, organizations can:
- Set defensible targets — "Reduce time-to-fill by 15% in FY26" is measurable only if FY25 time-to-fill is documented
- Align incentives to outcomes — structure retention bonuses that trigger when retention duration improves, not on arbitrary tenure milestones
- Meet funder evidentiary standards — New Jersey's 2026 RHT RFA requires quarterly progress reports and detailed personnel tracking; standardized baseline metrics satisfy these obligations without custom reporting overhead

Frequently Asked Questions
What is healthcare provider data management?
Healthcare provider data management is the systematic collection, organization, and maintenance of provider records — covering credentials, workforce metrics, location data, and availability — to support operational efficiency, compliance, and care coordination.
How is AI improving provider data management in 2026?
AI-native infrastructure automates data ingestion, deduplication, and quality monitoring across provider records, significantly reducing manual maintenance burden. Predictive analytics enable workforce planning by flagging burnout signals and forecasting vacancy timelines before crises emerge.
What are the biggest provider data challenges for rural healthcare organizations?
Rural facilities face fragmented systems with provider records scattered across platforms, limited IT staff to manage data quality, high provider turnover that quickly outdates rosters, and the absence of standardized workforce metrics for benchmarking or grant reporting.
What does FHIR compliance mean for rural health providers in 2026?
By January 1, 2026, rural providers must adopt FHIR-based API connections with payers, patients, and referral partners to meet CMS interoperability requirements. FHIR (Fast Healthcare Interoperability Resources) is the federal standard governing real-time health data exchange.
What HCP workforce metrics should rural healthcare organizations track?
Key metrics to monitor include:
- Vacancy rates by provider role (MD, NP, PA)
- Time-to-fill open positions
- Retention duration (median years per role)
- Compensation benchmarks relative to regional peers
- County-level access quality measures weighted for geography and population density
What is an outsourced data infrastructure model and is it right for rural healthcare?
Outsourced data infrastructure means a third party manages the data warehouse, AI pipelines, and analytics layer, giving rural organizations full HCP data capabilities without needing internal data engineering teams. For facilities with limited IT resources, this model provides immediate access to tools that were previously out of reach for smaller health systems.