Introduction
Three forces collided in 2026 to make healthcare claims data integration a deadline, not a discussion. CMS-0057-F prior authorization workflow requirements took effect January 1, 2026, with full API implementation required by 2027. The 2024 Change Healthcare ransomware attack exposed approximately 190 million patient records—the largest healthcare breach on record—showing exactly how fragmented systems amplify attack surface and recovery costs.
Meanwhile, the pressure to demonstrate value-based care outcomes keeps mounting. In rural markets, where 41.2% of hospitals operate with negative margins, that pressure demands data environments capable of supporting predictive analytics, population health management, and real-time utilization tracking.
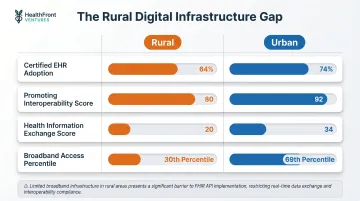
Most healthcare organizations—especially rural ones—still run fragmented, siloed claims systems that can't meet these demands. Rural providers face the steepest climb: 64% EHR adoption versus 74% urban, Health Information Exchange scores of 20 versus 34, and median operating margins of just 2.0%.
These organizations have neither the technical infrastructure nor the financial buffer to absorb compliance penalties, breach recovery costs, or missed value-based care opportunities.
This article covers what claims data integration actually means, why 2026 changed the stakes, and how rural healthcare organizations can build toward a connected data environment—even with constrained resources.
TLDR
- Claims data integration unifies medical, pharmacy, eligibility, authorization, and billing data into a governed system that supports clinical and financial decisions
- CMS-0057-F workflow compliance became active January 1, 2026, requiring 72-hour urgent and 7-day standard prior authorization responses
- The Change Healthcare breach affected ~190 million individuals, exposing how fragmented systems magnify cybersecurity risk
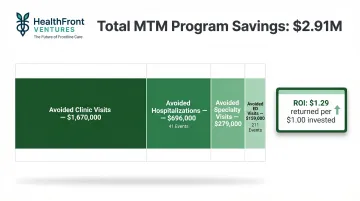
- Integrated claims unlock care coordination that reduces readmissions by 10-14%, plus MTM programs delivering $1.29 ROI per $1.00 invested
- Rural organizations face compounded barriers yet have the most to gain from purpose-built infrastructure like HealthFront Baseline™
What Is Healthcare Claims Data Integration?
Healthcare claims data integration consolidates medical claims, pharmacy claims, prior authorization records, eligibility data, adjudication results, and payer-provider billing transactions into a single, governed environment.
This goes far beyond simple data exchange. Integration requires normalization of inconsistent formats, standardization of code sets, resolution of patient and provider identities across systems, and consistent access across clinical and administrative workflows.
Integration Versus Interoperability
Interoperability means systems can exchange data using shared standards like FHIR and HL7. Integration takes it further—ensuring the resulting data is trustworthy, consistent, and analytically usable. Both matter, but integration is where real operational and clinical value is realized.
A payer system and a provider EHR can achieve interoperability by transmitting a claims file via FHIR API. But if the receiving system can't match the patient identity or normalize procedure codes, the data stays siloed. Integration applies governance rules, identity resolution, and data quality checks that transform raw transactions into a unified view.
Core data types consolidated through claims integration include:
- Medical claims: ICD-10 diagnoses, CPT/HCPCS procedures, Part A inpatient and Part B outpatient encounters
- Pharmacy claims: NDC codes, dispensing records, Part D data
- Prior authorization records: approval status, denial reasons, clinical justification
- Eligibility and benefits data: coverage verification, formulary details
- Adjudication and remittance: payment status, denial codes, adjustment reasons
- Payer-provider billing transactions: 837 claims submissions, 835 remittance advice
Organizations that unify these streams gain a longitudinal view of each patient's care history, financial interactions, and treatment patterns. That visibility drives more effective care coordination, stronger fraud detection, and more accurate population health analysis.
Why 2026 Is a Critical Turning Point
Federal Mandates Are Now Non-Negotiable
CMS-0057-F (Prior Authorization Rule) establishes a two-phase compliance timeline that directly affects every impacted payer—Medicare Advantage organizations, Medicaid and CHIP managed care plans, and Qualified Health Plan issuers on Federally Facilitated Exchanges.
Phase 1 - Active as of January 1, 2026:
Payers must respond to prior authorization requests within 72 hours for urgent cases and 7 calendar days for standard requests. Manual, siloed claims systems cannot meet this pace. Organizations must also begin publicly reporting prior authorization metrics on their websites, with the initial report due March 31, 2026, and submit annual Patient Access API usage metrics to CMS.
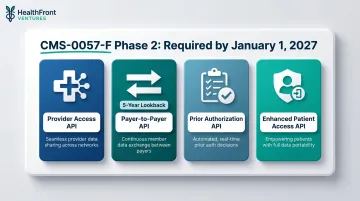
Phase 2 - Required by January 1, 2027:
Full implementation of four FHIR R4.0.1-based APIs is mandatory:
- Provider Access API: Shares claims, encounter data, USCDI data, and prior authorization information with in-network providers
- Payer-to-Payer API: Exchanges data with a five-year lookback when members switch plans
- Prior Authorization API: Supports electronic requests and responses with structured denial reasons
- Enhanced Patient Access API: Adds prior authorization status to member-facing portals
Organizations with disconnected systems face both compliance risk and member trust erosion when data isn't portable or current.
CMS-9115-F (Patient Access Rule) requires payers to make claims and encounter data accessible to members through secure, standardized APIs. This foundational requirement, combined with CMS-0057-F's extensions, means integrated, API-capable claims systems are now a compliance necessity, not just an operational improvement.
TEFCA Version 2.1 (updated October 9, 2025) establishes FHIR-based exchange as the default for qualified health information networks. The framework creates a "network of networks" model connecting providers, payers, public health agencies, and patients. While not universally mandatory, TEFCA alignment with CMS API requirements creates strong incentives for participation through designated QHINs. For rural organizations, QHIN partnerships offer a practical path to meet both TEFCA and CMS interoperability requirements simultaneously.
The Cybersecurity Imperative
The February 21, 2024 ransomware attack on Change Healthcare—a UnitedHealth Group subsidiary—remains the largest healthcare data breach on record and a clear illustration of the risks centralized, fragmented claims processing creates.
The breach affected approximately 190–192.7 million individuals. Change Healthcare processes 15 billion transactions annually and touches 1 in every 3 patient records in the US — serving as the backbone for more than 100 critical functions, from eligibility verification to payment processing.
The financial damage was severe:
- 94% of surveyed hospitals reported financial impact (American Hospital Association)
- 33% experienced disruption to more than half of their revenue
- Claims submissions dropped $6.3 billion in the first three weeks across 1,850 hospitals and 250,000 physicians
- 60% of hospitals needed two weeks to three months to resume normal operations
- Optum/UHG ultimately paid a $22 million ransom
The attack succeeded through compromised credentials on a Citrix portal without multi-factor authentication. There was a nine-day gap between initial intrusion (February 12) and discovery (February 21) — time enough for attackers to move laterally across interconnected systems. Post-acquisition integration failures after UnitedHealth Group's 2022 purchase of Change Healthcare compounded the exposure.
Consolidated, governed data environments with zero-trust architecture and continuous audit logging reduce the attack surface and enable faster breach containment than sprawling, siloed systems. The AHA specifically identified vendor redundancy and diversification as key factors determining which organizations recovered fastest.
Rural hospitals faced the sharpest exposure. With median cash reserves of only 29 days, they had almost no buffer to absorb weeks-long claims processing disruptions.
Key Benefits of Integrated Claims Data
For Patients and Care Teams
Enhanced care coordination: When medical and pharmacy claims are unified, every provider in a patient's care network sees the same complete picture — eliminating duplicate tests, conflicting prescriptions, and care gaps that surface when specialists work from incomplete data. Medicare readmission rates declined from 19.0% to 18.4% following increased coordination with outpatient providers supported by integrated claims visibility, with per-beneficiary readmissions running 10-14% lower in 2012 than in 2007.
The financial stakes are concrete: the CMS Hospital Readmissions Reduction Program (HRRP) penalized hospitals $521 million in FY 2022 for excess readmissions, making claims-driven coordination a compliance priority, not just a clinical one.
Better medication management: Integrated pharmacy and medical claims surface non-adherence patterns and flag dangerous drug interactions invisible in siloed systems. This enables early intervention and supports Medication Therapy Management (MTM) programs. A 10-year MTM study across 9,068 patients documented $2,913,850 in total savings ($86.45 per encounter) and an ROI of $1.29 per $1.00 invested. Savings broke down as:
- $1.67M from avoided clinic visits
- $696K from 41 avoided hospitalizations
- $279K from avoided specialty visits
- $159K from 211 avoided ED visits
For Health Systems, Payers, and Administrators
Cost reduction through unified data: Integrated claims support more accurate utilization management, reduce unnecessary procedures, and enable MTM programs that lower total cost of care. Organizations that connect pharmacy and medical data streams see measurable returns — and that ROI compounds when predictive tools enter the picture.
Predictive analytics and population health management: Unified claims data feeds risk-stratification models that identify high-cost or high-risk patients before costly events occur. The healthcare predictive analytics market was valued at $14.58 billion in 2023 and is projected to reach $67.26 billion by 2030, growing at a 24.0% CAGR. Population health management is the fastest-growing segment at 24.4% CAGR. Organizations that integrate claims data now position themselves to deploy predictive tools as the market matures and costs decline.
Fraud detection and accurate reporting: A consolidated claims environment makes anomalies, such as duplicate submissions, upcoding, and billing mismatches, detectable in near real time rather than through post-payment audits. This supports both regulatory reporting accuracy and audit readiness, reducing exposure to compliance penalties and overpayment recovery actions.
The Rural Healthcare Gap: Why Integration Is Even More Urgent Here
Rural healthcare organizations face compounded integration barriers that urban systems don't: limited in-house IT capacity, aging single-facility EHR systems with poor API support, thin operating margins that rule out custom data infrastructure builds, and geographic fragmentation that makes multi-site data coordination especially difficult.
Financial Fragility
The national median operating margin for rural hospitals is 2.0%, but 41.2% operate with a negative margin. In non-Medicaid-expansion states, the median drops to -0.7%, with 52.2% of hospitals in the red. Currently, 417 rural hospitals are vulnerable to closure, led by Texas (50), Kansas (44), and Tennessee (27). Critical Access Hospitals carry a median of only 29 days cash on hand.
Digital Infrastructure Gap
The technology deficit compounds the financial picture. Key disparities include:
- Certified EHR adoption: 64% rural versus 74% urban, with rural physicians showing 21% lower odds of adoption
- Promoting Interoperability Score: rural median 80 versus urban 92
- Health Information Exchange scores: 20 rural versus 34 urban
- Broadband access: rural residents rank at the 30th percentile versus the 69th percentile for urban — a direct barrier to cloud-based FHIR API implementations
Workforce Crisis
Rural areas have approximately 30 physicians per 100,000 people versus 263 in urban areas. HRSA projects rural (nonmetro) supply adequacy at only 42% by 2038 versus 95% in metro areas. More than half of rural doctors are aged 50 or older, with a projected 23% decline by 2030 due to retirements.
These three compounding pressures — financial, digital, and workforce — are precisely where integrated claims data delivers outsized value.
Provider utilization patterns embedded in rural claims data reveal which specialties are undersupplied, which patient panels are growing beyond sustainable capacity, and where NP/PA recruitment would produce the greatest access improvement. These are insights invisible without integrated data. State-level Rural Health Transformation (RHT) programs depend on that integrated baseline to measure whether workforce investments are working. Without a unified data environment, performance measurement collapses into manual reporting, jeopardizing program accountability and future funding appropriations.
HealthFront Baseline™ addresses this gap directly. HealthFront Ventures' AI-native HCP Workforce Data Warehouses and Lakes are built for exactly this context: outsourced data infrastructure that eliminates custom builds, delivering four quantitative metrics plus one rural county quality measure for FY25 baseline data and Q1 2026 workforce tracking.
Resource-constrained rural organizations get the same analytical depth as large health systems — without capital investment in data infrastructure or specialized IT staffing.
Common Challenges and How to Overcome Them
Three challenges consistently surface in claims integration projects—each requiring a distinct approach to resolve without derailing operations or budgets.
Inconsistent Data Formats and Legacy System Dependencies
Different claims systems use proprietary formats, outdated HL7 versions, or flat-file batch transfers that resist real-time integration. The practical path forward is adopting FHIR R4-compliant APIs and modern integration platforms that wrap legacy systems rather than requiring full replacement.
Middleware solutions like Mirth Connect provide pre-built v2.x-to-FHIR conversion templates, letting organizations expose FHIR-compliant API layers without a complete system overhaul. This matters especially for rural organizations that cannot afford rip-and-replace implementations.
HIPAA Compliance Across Integrated Environments
As more systems connect and PHI flows across a broader surface area, governance must be embedded from the start—not retrofitted afterward. The Change Healthcare breach demonstrated how compromised credentials and inadequate MFA can expose massive data volumes.
Core safeguards include:
- Role-based access controls and zero-trust architecture
- Encryption in transit and at rest
- Continuous audit logging
- Least-privilege access models with network segmentation
- Ongoing monitoring for anomalous access patterns

Patient Identity Matching Errors
When demographic data varies across payer, provider, and pharmacy systems, integrated records get split or incorrectly merged—corrupting downstream analytics. Only 22% of organizations achieve a 1% or less duplicate record error rate, and misidentification costs the average facility $17.4 million per year in denied claims and lost revenue.
Identity resolution needs to happen before data is combined, not as a cleanup task afterward. AHIMA's ICMMR Cycle (Identify, Clean, Measure, Mitigate, Remediate) offers a structured framework for reaching—and sustaining—that 1% duplicate target.
Frequently Asked Questions
What is medical claims integration?
Medical claims integration consolidates data from medical, pharmacy, eligibility, and billing systems into a unified environment. Providers and payers gain a complete view of a patient's care history and financial interactions in one place, enabling coordinated care decisions and accurate population health analytics.
How does an HIE differ from an EHR?
An EHR (Electronic Health Record) is a digital record system used by a single provider or health system to document patient care. An HIE (Health Information Exchange) is a network that lets multiple organizations share patient data across different EHR systems and care settings—supporting coordination across organizational boundaries.
What are the biggest barriers to claims data integration for rural health organizations?
Limited IT staffing, aging EHR systems with poor API support, thin operating margins that make custom infrastructure prohibitive, and geographic fragmentation are the primary barriers. Outsourced, purpose-built data infrastructure like HealthFront Baseline™ is the most practical path forward for most rural organizations, eliminating upfront capital costs and ongoing maintenance burdens.
How does claims data integration support provider workforce planning?
Integrated claims reveal provider utilization patterns, patient panel sizes, specialty gaps, and access bottlenecks. That data gives healthcare organizations and state programs what they need to target NP/PA recruitment, structure retention incentives, and measure the impact of workforce investments with documented outcomes rather than estimates.
Is claims data integration required for CMS compliance in 2026?
Yes. CMS-0057-F requires FHIR-based prior authorization workflows with a January 1, 2026 workflow deadline and January 1, 2027 API implementation deadline. CMS-9115-F requires standardized member access to claims data. Integrated, API-capable claims systems are now a compliance necessity, not just an operational improvement, for payers and health plans.
What is the difference between claims data integration and interoperability?
Interoperability refers to the ability of systems to exchange data using shared standards like FHIR and HL7. Integration goes further—normalizing formats, resolving patient identities, and applying governance rules so data is consistently usable for analytics, reporting, and clinical decisions. Without integration, interoperability delivers connectivity but not reliable, decision-ready data.