This article explains how healthcare data integration connects clinical, claims, workforce, and social determinants of health data into a coherent foundation for patient population analytics — and why the rural context demands a fundamentally different approach than urban-focused solutions.
Key Takeaways
- Healthcare data integration aggregates clinical, claims, SDOH, and workforce data into a unified foundation for population analytics
- Rural health systems face distinct fragmentation challenges — lower EHR interoperability maturity, disconnected small facilities, and limited IT capacity
- Effective integration enables risk stratification, chronic disease management, care coordination, and proactive interventions
- Outsourced AI-native data infrastructure lets rural organizations generate usable population health insights — no custom build required
What Is Healthcare Data Integration for Population Analytics?
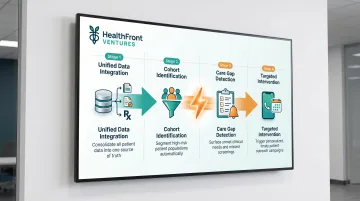
Healthcare data integration for population health is the process of pulling together data from disparate clinical, administrative, and social sources to create a unified, analytics-ready view of a defined patient population. This enables providers to flag risk early, track outcomes across cohorts, and coordinate care at scale — shifting from reactive, episode-based treatment to proactive population management.
Population Health vs. Clinical Analytics
Population health analytics differs from general clinical analytics in both scope and purpose. Where clinical analytics focuses on individual patient episodes, population health management focuses on cohorts — all diabetic patients in a county, all patients served by a rural FQHC, or all high-risk Medicare beneficiaries in a defined service area.
The goal is to inform proactive interventions that prevent deterioration and reduce avoidable utilization — not just to optimize treatment decisions once patients present for care.
According to the Centers for Medicare & Medicaid Services, a population health measure reflects the overall health and well-being of a group, covering topics including access, outcomes, coordination, behaviors, prevention, and utilization.
Why Rural Health Systems Need This More Than Most
Rural communities carry a disproportionate chronic disease burden. CDC data from 2025 shows diabetes prevalence among rural adults reached 14.3% versus 11.2% in urban settings in 2021, drawn from 378,504 observations across 41 states.
Rural residents are also more likely to die prematurely from the five leading causes of death:
- Heart disease
- Cancer
- Stroke
- Unintentional injuries
- Chronic lower respiratory disease
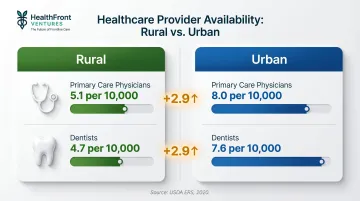
At the same time, rural areas have far fewer providers to manage this higher disease burden. USDA Economic Research Service data shows that primary care physicians per 10,000 residents in rural areas stood at just 5.1 versus 8.0 in urban areas as of 2020. Dentists per 10,000 were similarly scarce: 4.7 rural versus 7.6 urban.
| Provider Type | Rural (per 10,000) | Urban (per 10,000) |
|---|---|---|
| Primary Care Physicians | 5.1 | 8.0 |
| Dentists | 4.7 | 7.6 |
Without integrated data infrastructure, rural healthcare organizations have no reliable way to see where that gap is widest — or where targeted interventions would have the greatest impact.
Key Data Sources That Power Rural Population Analytics
Clinical EHR and Encounter Data
Electronic health records are the primary source of clinical truth — diagnoses, lab results, medications, vitals, and visit history. EHR data provides the clinical detail needed to understand patient health status, monitor chronic conditions, and track care delivery over time.
Rural settings, however, often operate multiple disconnected EHR instances. A critical access hospital may run one system while affiliated primary care clinics run another, and specialty providers may operate on entirely separate platforms. This fragmentation makes normalization and deduplication prerequisites — without them, aggregated records produce unreliable insights and missed care coordination opportunities.
Claims and Payer Data
Claims data fills critical gaps in clinical records by capturing out-of-network utilization, prescription fills, and specialist visits that don't appear in a provider's own EHR. For rural populations enrolled in Medicare or Medicaid, claims data is often the only complete longitudinal record available.
Medicaid covers approximately 24% of people living in rural areas compared to 21% in urban areas, according to KFF. Among rural Medicaid enrollees under age 65, 38% have at least one diagnosed chronic condition. This high prevalence, combined with the longitudinal completeness of claims data, makes payer data essential for rural population health analytics.
Social Determinants of Health (SDOH) Data
Rural SDOH profiles differ materially from urban ones. Transportation barriers, food deserts, housing instability, and limited broadband access all affect health outcomes — and these barriers are more severe in rural communities than in urban ones.
Federal Reserve Bank of Richmond analysis found that fixed wireline broadband in rural high-needs areas covers just 51–53% of households, versus 73% nationally. Adults in rural counties are also 42% less likely to use telehealth than urban residents. Device ownership compounds the gap:
- Smartphones: 76% rural vs. 88% nationally
- Laptops: 60% rural vs. 79% nationally
- Tablets: 48% rural vs. 63% nationally
Food insecurity compounds these access barriers. According to Feeding America's 2025 Map the Meal Gap report, over 80% of U.S. counties with the highest child food insecurity rates are rural, with some rural counties estimating child food insecurity as high as 50%.
Integrating these SDOH signals into population analytics shifts the focus from treating illness after it occurs to intervening on the conditions that drive it.
Healthcare Workforce and Provider Availability Data
Provider-to-patient ratios, NP/PA coverage gaps, and HCP retention metrics directly affect whether care plans can actually be executed — yet workforce data is frequently absent from urban-focused analytics platforms. For rural health organizations, this blind spot is consequential: population health programs designed without workforce visibility risk prescribing interventions the local infrastructure simply cannot deliver.
HealthFront Ventures' HealthFront Baseline™ is built specifically for this problem. Launching Q1 2026, it provides four quantitative workforce metrics plus a Rural County Quality Measure — giving rural health organizations a standardized baseline to align population health interventions with current and projected provider capacity.
Remote Monitoring and Patient-Generated Data
Wearables and home monitoring devices — glucose monitors, blood pressure cuffs, pulse oximeters — represent emerging data sources that extend the clinical picture between visits. This is particularly valuable in rural settings where patients may travel long distances for in-person care.
However, adoption remains uneven. Journal of Rural Health research found that remote patient monitoring for post-discharge care reached just 7% adoption among rural hospitals versus 23% among metropolitan facilities. Wider rural gaps exist for tele-stroke, psychiatric/addiction treatment, and ICU telehealth services. Integration challenges, digital literacy barriers, connectivity gaps, and staffing shortages all slow rural implementation.
How Data Integration Enables Patient Population Health Management
Risk Stratification and At-Risk Population Identification
Integrated data allows organizations to segment patient populations by risk level using signals like A1C values, ED visit frequency, medication adherence rates, and SDOH risk scores. This identifies which patients need proactive outreach before a preventable crisis occurs.
Research published in the Journal of the American Medical Informatics Association found that activation of hospitalization event notifications for Medicare fee-for-service beneficiaries in the Bronx was associated with a 2.9 percentage point reduction in 30-day readmissions — from 29.5% to 26.5% unadjusted — across a cohort of 2,559 beneficiaries and 14,141 admissions between 2010 and 2014. The study was conducted in an urban setting, but the mechanism — timely, event-driven notifications routed to care teams — translates directly to rural populations with high readmission risk.
Chronic Disease Management at Scale
Structured chronic disease programs become achievable when clinical, pharmacy, and claims data are unified across a defined geography. Care managers can see exactly which patients have gaps in monitoring, missed refills, or overdue follow-ups — and act before conditions deteriorate.
In rural settings, this cohort-based approach is not optional — it's a staffing necessity. Small care teams cannot manage high-risk populations one patient at a time. Automated identification of care gaps lets those teams concentrate effort where it has the greatest clinical impact.
Care Coordination and Post-Discharge Follow-Up
Seamless data integration between hospital discharge systems, primary care EHRs, and care management platforms enables timely follow-up after acute events — a critical gap in rural settings where patients may be discharged to communities with limited follow-up resources.
Admission, Discharge, Transfer (ADT) feeds are the core signal for care coordination workflows. Real-time ADT alerts allow care managers to initiate outreach calls, schedule follow-up appointments, and confirm medication reconciliation immediately after discharge, reducing the likelihood of readmission.
Proactive Intervention and Population Outreach
Targeted outreach becomes systematic — not ad hoc — when data is unified across the care continuum. Common outreach actions include:
- Automated reminders for overdue preventive screenings
- Care gap closure alerts routed to the responsible care manager
- High-risk patient lists generated by predictive models for proactive contact
The value of integration lies not just in analytics visibility but in closing the loop between insight and action.
For example, an integrated system can identify all diabetic patients in a defined population who have not had an A1C test in the past six months, generate outreach lists for care managers, and track completion rates. This transforms analytics from passive reporting into active intervention.
Performance Measurement Against Benchmarks
Tracking performance under value-based care contracts and state-level Rural Health Transformation programs requires reliable, population-level quality metrics. Integrated data makes that possible across measures such as:
- Colorectal cancer screening rates
- Blood pressure control in hypertensive populations
- 30-day readmission rates by discharge diagnosis
Without a unified data foundation, organizations cannot calculate these metrics consistently, benchmark against regional or national peers, or demonstrate improvement over contract periods. For rural organizations operating under thin margins, that accountability gap has real financial consequences.
Unique Challenges for Rural Healthcare Data Integration
Data Fragmentation Across Disconnected Systems
Rural health organizations often operate a patchwork of legacy EHRs, paper-based workflows, standalone lab systems, and unaffiliated specialty providers — creating deep data silos. Unlike large health systems with centralized IT infrastructure, rural CAHs and FQHCs rarely have dedicated integration engineers.
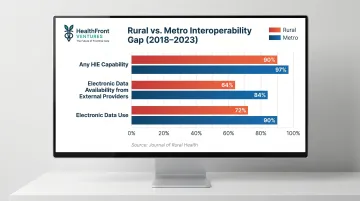
Journal of Rural Health data shows that hospitals reporting any health information exchange capability stood at 90% rural versus 97% metropolitan. Electronic data availability from external providers was 64% rural versus 84% metro, and electronic data use was 72% rural versus 90% metro. These gaps, measured from 2018 to 2023, show persistent rural disadvantages in interoperability maturity.
Interoperability and Standards Compliance
Semantic interoperability means data doesn't just move between platforms — it carries consistent meaning on both ends. FHIR (Fast Healthcare Interoperability Resources) and HL7 (Health Level Seven) define that standard, but many legacy rural systems predate them, requiring translation layers or middleware to bridge the gap.
Without consistent vocabulary standards, aggregated data produces unreliable analytics. The core vocabularies at stake:
- LOINC — standardizes lab and clinical observations
- SNOMED CT — standardizes condition and diagnosis coding
- RxNorm — standardizes medication naming across systems
A diabetes diagnosis coded in one system may not match the same diagnosis in another, leading to undercounting of chronic disease prevalence and missed care opportunities.
JAMIA research found that critical access hospitals (CAHs) lagged in adoption of advanced EHR functions. Bulk data export for population health reached 47% of CAHs versus 63% of non-CAHs in 2023. FHIR API support for patient apps stood at 65% CAHs versus 72% non-CAHs. These gaps in standards adoption make integration harder for the organizations that need it most.
Workforce Data Gaps Compounding Clinical Data Gaps
In rural population health management, the provider infrastructure itself is a variable — not a fixed baseline. When NP and PA vacancies go unfilled, care plans stall regardless of how precise the analytics are.
Most population health platforms treat workforce as a static input. In rural health, it's a dynamic constraint that belongs inside the analytics model. Without integrating workforce availability metrics into population health planning, organizations risk designing interventions that exceed local delivery capacity.
Privacy, Security, and Compliance in Resource-Constrained Environments
HIPAA compliance, state-level data privacy regulations, and consent management for SDOH data create a compounding compliance burden, and rural organizations rarely have dedicated compliance or security teams.
HIPAA Journal analysis of HHS data shows that 742 large healthcare data breaches affecting 500 or more individuals were reported in 2024, with cumulative breaches from October 2009 to January 2026 totaling 7,419. While rural-specific breach costs are not separately tracked, the regulatory consequences of non-compliance are identical regardless of organization size.
Outsourced data infrastructure can embed compliance controls without requiring rural organizations to build them from scratch, reducing both risk and operational burden.
Analytics Frameworks That Turn Integrated Data into Action
Cohort-Based Analytics: Start with the Population, Not the Platform
Before configuring dashboards or pipelines, define the patient population by condition, geography, risk level, or payer type. This cohort definition drives what data must be integrated, what signals to track, and what actions to trigger — preventing the common mistake of building data infrastructure without a clear use case.
Measure, Act, Prove: A Repeatable Framework for Rural Population Health Programs
Three steps convert integrated data into measurable outcomes:
- Measure: Define the signals and quality rules for each cohort — A1C values, follow-up completion rates, and similar condition-specific indicators.
- Act: Wire specific responses to threshold breaches, including outreach calls, care management escalations, and scheduling triggers.
- Prove: Track acknowledgment rates, completion, and outcome shifts to build the evidence base for program continuation and funding.

Rural health programs accountable to state-level RHT funders face direct pressure to show measurable returns — this sequence creates the audit trail that justifies ongoing investment.
Key Metrics That Matter for Rural Population Health Analytics Dashboards
Rural health program leaders should track:
- First-pass data quality yield: What percentage of incoming records clear validation without manual correction
- Event-to-insight latency: Minutes or hours between a clinical event and its appearance in analytics
- Care gap closure rate by cohort: How effectively the program is resolving identified gaps across each population segment
- 30-day readmission rate: A direct indicator of care transition quality and post-discharge follow-through
- Provider availability coverage: Active NP/PA/MD capacity relative to total enrolled population
These metrics bridge clinical performance and operational capacity in a way that standard population health management dashboards often miss.
Building a Sustainable Data Foundation for Rural Health
The build-versus-buy reality for rural healthcare organizations is stark. Custom data integration infrastructure demands resources most rural health systems simply don't have:
- Engineering talent for design, deployment, and upkeep
- Ongoing maintenance as healthcare data standards evolve
- Compliance oversight across HIPAA and state-level reporting requirements
- Capital investment that competes directly with clinical staffing budgets
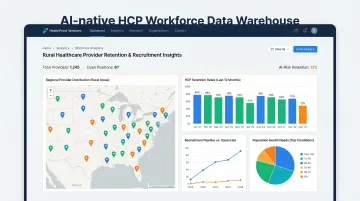
Outsourced, AI-native data warehouse and data lake solutions eliminate this burden — giving rural organizations access to enterprise-grade population health analytics without the overhead.
HealthFront Ventures addresses this need directly through AI-Native HCP Workforce Data Warehouses and Lakes designed specifically for rural healthcare provider retention and recruitment programs. This enables organizations to act on workforce-informed population analytics through a managed infrastructure model — avoiding the cost and complexity of custom builds while maintaining the reporting depth required for value-based care contracts.
That infrastructure advantage matters beyond cost savings. As state-level Rural Health Transformation programs increasingly require data-driven accountability, organizations with integrated data foundations are better positioned to demonstrate outcomes, secure continued funding, and sustain the provider workforce needed to deliver on population health goals. Getting that foundation in place early — rather than scrambling to retrofit it when reporting deadlines arrive — is what separates programs that scale from those that stall.
Frequently Asked Questions
What data sources are most important for rural patient population analytics?
The four primary categories are clinical EHR and encounter data, payer and claims data, SDOH data specific to rural contexts (transportation, food access, broadband connectivity), and healthcare workforce data. Each addresses a distinct dimension of population health, so all four are necessary to capture a complete risk picture in rural communities.
How does healthcare data integration differ for rural versus urban health systems?
Rural data integration faces greater fragmentation across unconnected small facilities, lower EHR interoperability maturity, the added dimension of workforce scarcity as a population health variable, and limited in-house IT capacity to manage integration infrastructure. Rural organizations also face higher chronic disease burdens with fewer providers, making effective integration more urgent but harder to achieve.
What are the biggest technical challenges in healthcare data integration for population analytics?
The top barriers are achieving semantic interoperability across systems using standards like FHIR and HL7, maintaining data quality and consistency across disparate sources, and managing HIPAA-compliant security and consent workflows — all while operating with limited IT resources. Without consistent vocabulary standards, aggregated data produces unreliable analytics that undermine decision-making.
How does healthcare workforce data factor into patient population health analytics?
In rural settings, provider availability — NP, PA, and MD coverage levels — directly determines whether care plans built from population analytics can actually be delivered. Workforce metrics are a planning input, not just an operational concern: capacity gaps create hard ceilings on intervention scalability no matter how strong the underlying analytics are.
What is the minimum viable dataset needed to start population health analytics for a rural cohort?
Start with these core elements:
- Patient demographics and contact information
- Encounter history and discharge dispositions
- Active diagnoses and medications
- Key lab values such as A1C and blood pressure
- Insurance and coverage status
- At least one SDOH screening indicator for the target cohort
This foundation supports basic risk stratification and care gap identification before expanding to more complex datasets.
Can small rural healthcare organizations realistically implement healthcare data integration without large IT teams?
Yes. Outsourced and managed data infrastructure solutions now make this achievable. AI-native platforms designed for rural health contexts handle the technical complexity — including standards compliance, data pipeline management, and security controls — so rural organizations can focus on using the analytics rather than building the infrastructure.