Introduction
Rural America faces a stark healthcare access gap: roughly 20% of Americans live in rural areas, yet these communities hold only a fraction of the nation's physician workforce. 92% of rural counties were designated wholly or partially as primary care Health Professional Shortage Areas (HPSAs) in 2023 — a designation that reflects chronic, structural underservice.
The numbers on the ground are equally stark. 45% of rural counties have five or fewer primary care physicians, and 199 rural counties have none at all.
The situation is worsening, not stabilizing. More than one-third of currently active physicians will be 65 or older within the next decade, and rural communities will absorb an outsized share of those retirements.
HRSA projects rural primary care supply will meet only 68% of demand by 2037. Nationally, the physician shortage could reach 141,160 FTE by 2038.
This article examines emerging solutions across workforce pipelines, incentive design, care models, and data infrastructure — approaches that are producing measurable change in rural staffing outcomes.
Key Takeaways
- Rural shortages stem from provider maldistribution, not just supply—solutions must address why clinicians don't go and why they don't stay
- Building sustainable pipelines starts early: rural background and rural residency exposure are stronger predictors of rural practice than post-graduation incentives alone
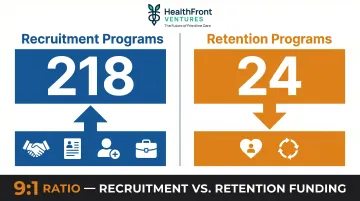
- Loan repayment dominates recruitment spending, but retention is chronically underfunded—24 retention programs nationally vs. 218 recruitment programs
- Advanced practice providers and telehealth expand capacity, but both require scope-of-practice modernization and broadband infrastructure to deliver
- Baseline HCP workforce metrics separate effective programs from ineffective ones—organizations with this data allocate incentives better and can demonstrate ROI
Why Rural Staffing Shortages Are Getting Worse, Not Better
The Maldistribution Problem
The rural physician shortage is fundamentally a distribution failure. Rural counties average one physician per 2,881 residents, with stark regional variation—from 3,411:1 in the South to 1,979:1 in the Northeast. Urban areas consistently maintain higher provider-to-population ratios, revealing that the problem isn't simply national physician supply—it's where physicians choose to practice.
HRSA's 2025 workforce analysis projects that non-metro areas will experience greater shortages than metro areas as population aging and physician retirements compound existing gaps. Meanwhile, 63.1% of designated primary care HPSAs are in rural areas, underscoring how shortage burdens fall disproportionately outside metropolitan regions.
The Demographic Time Bomb
The rural physician workforce is aging faster than replacements are arriving. AAMC projections show that more than one-third of currently active physicians will be 65 or older within the next decade, driving a retirement wave that will stress rural access where coverage is already thin. By 2036, the U.S. could face a shortage of 13,500–86,000 physicians nationally, with rural communities absorbing an outsized impact.
Why Rural Communities Can't Compete
Those vacancies don't fill themselves—and rural communities face structural barriers that make recruitment a losing battle against urban systems. Recruitment and retention literature consistently documents five pressure points:
- Earns less despite equal debt: rural compensation remains compressed relative to urban peers, even for physicians carrying identical medical school loan burdens
- Cuts off professional development: limited access to CME, peer networks, and career advancement infrastructure makes rural practice feel like a dead end
- Offers fewer clinical pathways: lower case volumes and minimal specialization opportunities push training-stage physicians toward urban systems with structured career ladders
- Creates operational friction: telehealth payment parity gaps, broadband deficiencies, and patient transportation barriers add administrative burden urban practices don't face
- Skips rural entirely in training: fewer rural rotations and residency programs mean most physicians finish training without ever practicing outside a metropolitan setting

Without intervention at the data and planning level, these barriers compound over time—making each retirement harder to replace than the last.
Building the Workforce Pipeline From the Ground Up
The Case for Early Intervention
The strongest predictor of rural practice isn't financial incentives—it's early rural exposure. Research using national family physician data shows that rural background physicians choose rural practice 39.2% of the time, compared to just 13.8% for urban background physicians. Rural residency training amplifies this further: 50.9% of rural residency trainees choose rural practice versus 18.0% of urban residency graduates.
The combined effect is decisive. Physicians with both rural background and rural residency training choose rural practice 82.7% of the time — compared to just 12.5% for those with urban background and urban residency.
Yet most current programs don't intervene until medical school or later—missing the window when career identity and intent are forming.
The High School Partnership Model
York General Hospital and York Public Schools in Nebraska demonstrate how early pipeline development works in practice. Since 2016, more than 150 high school students have participated in the program, logging over 10,000 clinical hours across hospital and clinic settings. Reported outcomes include scholarships, entry into clinical training programs, and multiple participants returning as employees.
The "homegrown pipeline" model works because participants already understand rural community life before they enter training. Small rural hospitals don't need large budgets to replicate it — structured clinical exposure during high school is the mechanism, and local relationships are the foundation.
Rural Residency Rotation Strategy
Sanford Health Bemidji embedded one-month rural rotations in emergency medicine and psychiatry within Hennepin Healthcare's urban residency program. The model creates intentional rural exposure pathways for physicians training in cities, with early results showing increased resident interest in Bemidji placements.
Brief rural exposure can shift career intentions even among physicians who never considered rural practice. For health systems that can't fund standalone rural residency programs, embedded rotations offer a lower-cost path to the same outcome — and a direct line into the recruitment pipeline.
AHEC Scholar Programs
Area Health Education Center (AHEC) Scholar Programs offer structured two-year pipelines combining didactic and experiential learning across six core areas:
- Interprofessional education
- Behavioral health integration
- Community connections
- Virtual learning and telehealth
- Practice transformation
- Current health issues
Programs that explicitly prefer rural-origin or in-state applicants consistently outperform those that don't. Yet only 20 of 247 programs reviewed stated a preference for rural-origin applicants, despite rural background being one of the strongest predictors of long-term retention.
The Retention-Recruitment Imbalance
Of the 247 programs reviewed in a comprehensive narrative analysis, only 24 focused on retention versus 218 on recruitment. This imbalance reveals a critical gap: most programs focus on placing providers, not keeping them.
A genuine pipeline strategy doesn't end at placement. Retention-specific interventions — continuing medical education support, leadership tracks, housing assistance, and structured professional development — consistently receive less funding than recruitment programs. Until that ratio shifts, rural health systems will keep refilling positions rather than building stable workforces.
Financial Incentives and Flexible Staffing Models That Drive Retention
Major Incentive Categories and Their Trade-offs
Loan Repayment Programs (LRPs): The National Health Service Corps (NHSC) LRP offers up to $75,000 for primary care physicians, NPs, CNMs, and PAs serving full-time (two years) at approved primary care HPSA sites, with up to $50,000 for other eligible disciplines. Half-time commitments receive proportional awards. The Students to Service LRP provides up to $120,000 disbursed in four annual installments contingent on service.
Awards are not taxable and can be extended through continuation contracts. LRPs are the most common incentive type among the 247 programs reviewed, with 70 programs using this mechanism.
J-1 Visa Waivers: The federal Conrad 30 program allows each state to waive the two-year home residency requirement for up to 30 J-1 physicians annually, typically deployed to HPSAs or Medically Underserved Areas. These waivers require a three-year service commitment but provide no additional financial incentive beyond the visa pathway itself. Forty-eight programs in the national review used J-1 waivers.
Scholarships: Twenty-six programs offer scholarships with lower dollar amounts than LRPs but earlier pipeline intervention. Scholarships target students before graduation, influencing career decisions at formative stages.
The Incentive Stacking Gap
Most scholarship recipients cannot simultaneously qualify for LRPs, creating a financial catch-22 where early-career commitments block access to the most generous post-graduation support. Complementary program design should allow students to layer scholarships with LRPs without penalty, maximizing support across the training continuum.
Surgicalist and Fractional Physician Staffing Models
Surgicalist and fractional physician staffing models are emerging as cost-effective alternatives to full-time hiring or locum tenens. Rural hospitals use them to access scheduled or rotational specialty coverage, including:
- Orthopedics
- General surgery
- Trauma
Early hospital administration reports indicate these models close critical specialty access gaps without the overhead of permanent recruitment. Peer-reviewed outcome data is still developing, but adoption is accelerating.
Retention-Specific Financial and Career Incentives
Retention programs are the most underfunded category, yet they're essential for long-term workforce stability. Retention-focused packages in practice include:
- Continuing medical education support and conference funding
- Leadership tracks and administrative career pathways
- Housing assistance and community integration resources
- Structured professional development and mentorship programs
FirstHealth of the Carolinas committed $20 million in capital investment to culture and career development, combining student sponsorships, apprenticeships, faculty stipends, internal academies, and culture initiatives like Walk in My Shoes and CEO listening sessions. The result: employee engagement restored to the 82nd percentile.

That result came from sustained, multi-layered investment — the kind of systemic commitment that one-time signing bonuses cannot replicate.
Rural Origin Preference as an Incentive Design Lever
Despite research showing rural background is one of the strongest predictors of long-term rural retention, only 20 of 247 programs reviewed stated a preference for rural-origin applicants. Funders and state programs should redesign eligibility criteria to weight this factor more heavily—targeting the candidates data consistently shows will remain.
Expanding Rural Capacity Through APPs and Telehealth
The NP/PA Workforce as an Underutilized Capacity Lever
Advanced practice providers—nurse practitioners and physician assistants—can deliver primary, emergency, and in some cases specialized care in rural settings, often supported by remote physician consultation. Thirty jurisdictions now grant full practice authority (FPA) to NPs, and states with FPA show measurably better rural access outcomes.
Scope-of-practice laws vary significantly by state, with direct consequences for rural deployment:
- Restrictive states require physician supervision or collaboration agreements, limiting NP autonomy and reducing placement flexibility
- Full practice authority states remove those barriers, allowing NPs to operate independently and fill gaps faster
- The gap is measurable — FPA adoption directly correlates with improved rural provider availability
What Telehealth Actually Does (and Doesn't) Solve
Telehealth meaningfully extends rural access to specialty and mental health care, enabling remote provider consultation and reducing patient travel burdens. Research shows broadband access and internet speed strongly correlate with telehealth use and primary care utilization.
The limits are just as real as the benefits:
- Cannot replace in-person care for diagnostic or procedural needs
- Broadband gaps suppress adoption — rurality and limited connectivity depress telemedicine uptake relative to better-connected communities
- Patient preference for in-person visits remains a genuine, underappreciated barrier
Telehealth is a complement to on-the-ground staffing — not a substitute for it.
The Interstate Medical Licensure Compact (IMLC)
Licensing friction is one reason telehealth's rural reach stays limited. The IMLC addresses that directly: it streamlines multi-state licensure, increasing the pool of physicians available to serve rural areas either remotely or through rotation-based models. Dozens of states now participate, though the total number of licenses issued via the compact and rural-specific deployment outcomes remain underdocumented in public reports.
Expanding IMLC participation reduces administrative friction for telehealth providers and enables physicians to cover multiple rural facilities across state lines more efficiently.
Team-Based Care as Structural Redesign
The University of Vermont Health Network centralized utilization management and physician advisor functions, deploying non-clinical tasks to remote roles across multiple states. This operational redesign ensured systemwide rural coverage with minimal staffing additions — a result no new hire alone could have produced.
Team-based care models redistribute workload, reduce clinician burnout, and extend existing provider capacity without requiring full-time recruitment for every function.
The Missing Piece: Measuring What Works with Workforce Data
Most Rural Health Organizations Lack Structured Workforce Data
The PMC narrative review explicitly noted that "limited program evaluation data" prevented conclusions about which incentives actually work. Most rural health organizations lack the data infrastructure to track HCP recruitment, retention, and turnover in any structured way — which means they can't identify which recruitment efforts deliver ROI, which retention programs reduce turnover, or where geographic gaps are widening. The result is reactive hiring instead of strategic workforce planning.
What a Workforce Data Baseline Looks Like in Practice
Quantitative metrics that matter for rural HCP workforce tracking include:
- Provider-to-population ratios by county and specialty
- Vacancy rates and time-to-fill for open positions
- Turnover rates and post-commitment retention percentages
- County-level quality measures tied to access and outcomes
HealthFront Ventures is launching HealthFront Baseline™ in Q1 2026, an AI-native workforce data solution providing FY25 Baseline Data Metrics across four quantitative measures plus one Rural County Quality Measure for MDs, NPs, and PAs in rural settings. With that foundation in place, organizations can move from anecdotal impressions to evidence-based workforce decisions — and that shift directly affects how incentive dollars get spent.
The Case for Data-Driven Incentive Planning
When rural health organizations have baseline workforce data, they can:
- Structure recruitment and retention incentives around actual vacancy patterns, not assumptions
- Target geographic areas of highest need with precision
- Demonstrate program ROI to state funders and federal grant programs
- Shift from reactive hiring to proactive workforce strategy
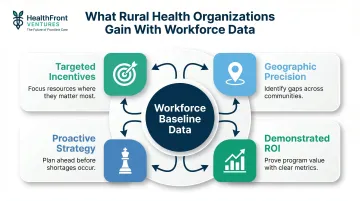
Organizations that track HCP workforce metrics allocate incentive dollars more effectively, justify budget requests with hard evidence, and measure the actual impact of pipeline and retention investments over time. Workforce data isn't overhead — it's the mechanism that makes every other rural staffing strategy work.
Policy and Advocacy Levers Worth Watching
Federal and State Funding Streams
Major federal programs supporting rural workforce development include:
- HRSA's National Health Service Corps (NHSC): Loan repayment and scholarship programs
- Nurse Corps: Funding for nursing education and loan repayment
- AHEC Scholar Programs: Pipeline development through structured experiential learning
- J-1 Visa Waiver Programs: State-administered Conrad 30 placements in HPSAs
CMS announced $50 billion in Rural Health Transformation (RHT) awards to strengthen rural health across all 50 states, allocated over five years at $10 billion annually. State examples include New Hampshire receiving over $204 million in 2026 and Maine receiving $190 million for Year 1.
At the state level, these appropriations are translating into concrete workforce programs — retention incentives, data infrastructure buildouts, and pipeline expansion tied to measurable HPSA reduction targets.
Scope-of-Practice Reform as the Highest-Leverage Policy Variable
Where funding streams set the budget, scope-of-practice law sets the ceiling on how that budget can actually deploy providers. Modernizing APP practice authority is the fastest regulatory path to expanding rural care capacity. States with full practice authority for NPs are more likely to have NPs practicing in rural and underserved areas, according to AANP policy analysis.
The core debate is whether NPs should require physician supervision or collaboration agreements. States moving toward full practice authority see measurable access improvements; restrictive states constrain NP deployment and slow capacity gains — a structural drag that no amount of federal funding can fully compensate for. States carrying both a large rural population and a severe HPSA burden have the most to gain from acting here.
Frequently Asked Questions
What is causing the rural healthcare staffing shortage?
The shortage stems from provider maldistribution, not just overall supply. Rural areas have far fewer physicians per capita than urban areas, compounded by an aging rural physician workforce, inadequate rural training pipelines, and financial and lifestyle factors that make urban practice more attractive to graduates carrying large debt loads.
How effective are loan repayment programs at retaining rural physicians long-term?
LRPs are the most common incentive type, but retention drops sharply once service commitments end. Research shows many physicians leave HPSAs when their contract is fulfilled, suggesting LRPs are better at initial placement than long-term retention. Sustained retention requires complementary investments in culture and career development, not financial incentives alone.
Can nurse practitioners and physician assistants fully address rural physician shortages?
NPs and PAs are a critical capacity expansion tool—particularly in primary care—but their impact depends heavily on state scope-of-practice laws, physician collaboration resources, and support infrastructure. They work best within a team-based care model, not as a standalone replacement for physicians.
What role does telehealth play in solving rural healthcare staffing gaps?
Telehealth extends rural access to specialty and mental health care and enables remote provider consultation, but broadband gaps and patient preference for in-person visits limit its reach. It works best as a complement to on-the-ground staffing, not a substitute for it.
How can rural hospitals measure whether their workforce strategies are actually working?
Most rural organizations currently lack standardized data infrastructure to track HCP recruitment, retention, and turnover metrics over time. Establishing a quantitative workforce baseline is the first step. Organizations that track vacancy rates, time-to-fill, and county-level provider ratios are better positioned to allocate incentive dollars effectively and demonstrate ROI to state and federal funders.
What federal programs currently support rural healthcare workforce development?
Key federal mechanisms include:
- HRSA's National Health Service Corps (loan repayment and scholarships)
- Nurse Corps program
- AHEC Scholar Programs
- J-1 Visa Waiver programs (administered by states)
- Rural Health Transformation NOFO grant funding from CMS
Availability and funding levels vary by state, and many high-need states remain under-served relative to their HPSA designation scores.