Introduction
Rural Oklahoma communities face a critical healthcare access crisis. All 77 counties experience mental health and primary care provider shortages, according to HRSA data, while 22 rural hospitals sit at immediate risk of closure within 2-3 years.
The problem extends beyond facilities. Oklahoma's rural residents contend with limited diagnostic equipment, inadequate telehealth infrastructure, and behavioral health services that reach fewer than one-third of those who need them. The pressure grew sharper when federal legislation enacted $911 billion in Medicaid reductions over the next decade, projected to cost Oklahoma hospitals $8 billion in lost revenue.
The Oklahoma Rural Health Transformation (RHT) Program represents the state's response : a share of a historic $50 billion federal investment distributed over five years. Oklahoma secured $223,476,949 for 2026 alone, ranking as the 5th-highest state award nationally. This funding targets fundamental transformation in how care is delivered, not simply offsetting Medicaid losses.
This guide covers what the program is, where the $223 million is deployed, who qualifies, how to apply, and what workforce-focused organizations need to prepare.
TLDR:
- Oklahoma secured $223.5 million in Year 1 funding from the $50 billion federal Rural Health Transformation Program
- Funding supports 29 distinct initiatives across telehealth, workforce development, behavioral health, and hospital stabilization
- 75 of 77 counties qualify as "rural" under program eligibility (all except Oklahoma and Tulsa counties)
- The first public microgrant program closed April 2026; a second funding opportunity (Rural Regional Reorientation) closes June 12, 2026
- Organizations need quantitative workforce baselines to qualify for retention and recruitment funding
What Is the Oklahoma Rural Health Transformation Program?
The Oklahoma RHT Program is a five-year cooperative agreement between Oklahoma and the Centers for Medicare & Medicaid Services (CMS), authorized under the One Big Beautiful Bill Act (H.R. 1). The national program allocates $50 billion to states from fiscal year 2026 through 2030, distributed at $10 billion annually across all 50 states.
Funding Structure and Oklahoma's Competitive Edge
Half of the $50 billion flows to states as equal baseline grants — approximately $100 million per state annually. The remaining half is awarded competitively based on application quality, rurality metrics, hospital financial conditions, and provider availability.
Oklahoma's $223.5 million award exceeds the $200 million national average by roughly $23.5 million — a competitive premium that reflects the strength of the state's demonstrated need and implementation plan.
Legal and Administrative Framework
As a cooperative agreement rather than a direct grant, funds flow through reimbursement mechanisms. Organizations cover costs upfront and submit documentation to receive payment — a structure that requires careful cash flow planning.
The Oklahoma State Department of Health (OSDH) serves as lead agency, coordinating with three project leads: the Oklahoma Health Care Authority, State Department of Education, and Healthcare Workforce Training Commission.
Sustainability and Accountability
States must plan to sustain investments beyond the five-year window. The federal accountability structure includes:
- Rollover rule: Unspent year-end funds carry forward; any remaining balance after the following year returns to the U.S. Treasury
- Quarterly and annual reporting to CMS on program progress
- Monthly coordination calls with CMS program staff
- Annual CMS Rural Health Summit participation required
Budget Period 1 runs through October 30, 2026. All funds must be obligated by that date and fully spent by September 30, 2027 — the close of federal fiscal year 2027.
How Oklahoma's $223 Million Will Be Deployed
OSDH published a Rural Health Transformation Program Initiative Funding Summary listing 29 distinct programs under six strategic categories. The breadth of initiatives spans everything from maternal-fetal medicine telehealth to EMS centralization, with funding allocations ranging from $800,000 to $43 million per program.
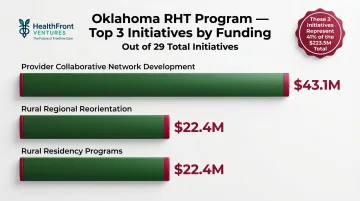
Top Three Funded Programs:
- Provider Collaborative Network Development: $43.1 million
- Rural Regional Reorientation: $26.4 million
- Rural Residency Programs: $22.4 million
These three programs account for over 41% of total funding — and together, they reveal where Oklahoma is placing its biggest bets: regional coordination and building a durable workforce pipeline.
Key Focus Areas
Healthcare Access and Infrastructure
The program prioritizes making care available where people live, work, and play. Eligible investments include:
- Emergency, primary, and specialty care services expansion
- Electronic health record system deployment
- Telestroke program infrastructure
- Clinical diagnostic equipment and telehealth carts (eligible under microgrants)
Telehealth and Broadband Expansion
Telehealth only works where connectivity exists — and Oklahoma still has ground to cover. Approximately 11% of locations lack adequate high-speed internet access, according to FCC Broadband Data Collection data. The Oklahoma Broadband Office's 2024 Annual Report targets 95% coverage by June 2028 through over $500 million in awarded grants, with 160 projects underway in 57 counties.
RHT Program partnerships with the Oklahoma Broadband Office address connectivity barriers that prevent telehealth adoption. The microgrant program explicitly lists telehealth carts and infrastructure as eligible uses — reflecting a practical acknowledgment that hardware alone can't close the access gap.
Behavioral Health Integration
Behavioral health integration into primary care is a named RHT initiative. ODMHSAS data indicates between 66–79% of Oklahomans with any mental illness do not receive treatment, with gaps even wider in rural areas. Program strategies include:
- Community health worker (CHW) expansion in hospitals
- School-based behavioral health services support
- Integration of mental health services into primary care workflows
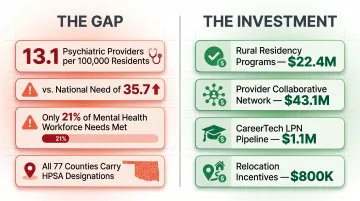
Oklahoma has only 13.1 psychiatric providers per 100,000 residents versus an estimated national need of 35.7 per 100,000 — the state would need to more than double its psychiatric residency slots to match the current national average within 10 years.
Workforce Development
Workforce development spans three major programs totaling $24.3 million:
- Rural Residency Programs: $22.4 million to expand MD and NP/PA training in rural settings
- CareerTech LPN "Grow Your Own": $1.1 million for licensed practical nurse pipeline
- HWTC Relocation Incentives: $800,000 for provider recruitment
All 77 Oklahoma counties carry HRSA designations for mental health and primary care provider shortages. The shortfalls are deepest in psychiatric and primary care specialties — a 2026 report found the state meets only 21% of its mental health workforce needs.
Hospital Stabilization
22 Oklahoma hospitals face immediate closure risk within 2–3 years, making stabilization one of the program's most urgent mandates. RHT funds are structured for long-term impact, not short-term relief:
- Eligible: Capital investments, infrastructure upgrades, network development
- Not eligible: Everyday operational expenses or services already covered by federal programs
Programs like Provider Collaborative Network Development ($43.1M) and Value-Based Care Enablement ($1.6M) target financial sustainability — addressing the structural conditions that put hospitals at risk in the first place.
Understanding Eligibility: Who Qualifies and What Counts as Rural
Before applying, note that Oklahoma's definition of "rural" is broader than the federal standard. Rural means communities and towns with populations under approximately 50,000 that are not located within Oklahoma County or Tulsa County — covering approximately 75 of the state's 77 counties.
Eligible Organizations:
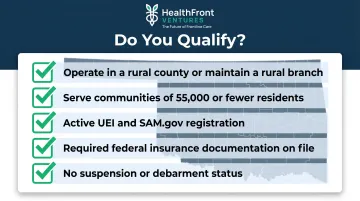
Nonprofits, independent healthcare provider practices, community organizations, and partner state agencies can participate. For the microgrants program specifically, organizations must:
- Operate in a rural county or maintain a branch serving one
- Serve communities with populations of 55,000 or fewer residents
- Hold active Unique Entity Identifier (UEI) and SAM.gov registration
- Carry required federal insurance documentation
- Not be suspended or debarred
Organizations outside rural areas may still qualify for certain initiatives, provided they clearly show how rural communities will be engaged as partners and how RHT funds will serve rural beneficiaries directly.
The Microgrants Program: Oklahoma's First Public Funding Opportunity
The Community-Led Wellness Hubs: Microgrants program (RHTP2026001) launched March 16, 2026, as the first public-facing Notice of Funding Opportunity under Oklahoma's RHT Program. Program Director Jackie Kanak stated this microgrant was "a direct result of what we heard during our listening sessions" — residents told the state that even small investments, like diagnostic equipment or wellness resources, could make meaningful differences in access to care.
Program Details:
- Total allocation: $3.75 million
- Award range: $50,000–$250,000 base; up to $50,000 supplemental per eligible county (max $250,000 supplemental)
- Application deadline: April 13, 2026 at 11:59 PM CT (now closed)
- Award notices: Late May to early June 2026
- Expenditure deadline: October 30, 2026
- Payment structure: Reimbursement-based
What Can Microgrant Funds Be Used For?
Eligible uses focus on one-time purchases of lasting assets:
- Clinical diagnostic equipment
- Telehealth carts and clinical access infrastructure
- Fitness and sports equipment (wellness enablers)
- Installable equipment or fixtures
- Health education and promotion materials
- Targeted subcontractor support
Funds CANNOT cover:
- Staffing or fringe expenses
- Student loan repayment programs
- Major facility renovations or structural changes
- New construction
- Broadband infrastructure
- Ongoing maintenance or subscriptions
- Food items, lobbying, or pre-award costs
Application and Award Timeline
The microgrants NOFO, supporting materials, and a downloadable eligible counties list are available at Oklahoma.gov/health/RHTPfunding. The April 13 deadline has passed; recipients must complete expenditures by October 30 and submit final invoices by November 30.
With the microgrant window closed, attention turns to the next funding round.
Second NOFO Now Active:
The Rural Regional Reorientation (RRR) program (RHTP2026002) is currently accepting applications with a June 12, 2026 deadline. This program offers grants up to $4 million per award, with $20 million total funding. The RHT funding page lists all active and upcoming NOFOs across the remaining 27 programs.
The Rural Healthcare Workforce Challenge RHT Aims to Solve
Oklahoma faces a severe healthcare provider shortage that threatens rural access to care. All 77 counties carry Health Professional Shortage Area (HPSA) designations for mental health or primary care. The state has significantly fewer psychiatric prescribers — 13.1 per 100,000 residents — compared to the national estimated need of 35.7 per 100,000. Rural areas face more acute shortages than urban centers, with limited access to physicians, nurse practitioners, and physician assistants across specialties.
The RHT Program addresses workforce challenges through:
- Rural residency programs ($22.4M)
- Workforce retention and recruitment incentives ($800K relocation support)
- Licensed practical nurse pipeline development ($1.1M CareerTech program)
- Provider collaborative network development ($43.1M for regional coordination)
Workforce Data Infrastructure
Sustainable workforce data infrastructure is essential for organizations to apply for, track, and report on workforce-focused RHT initiatives. Applications require quantitative baselines: current provider counts, retention rates, geographic coverage gaps, and productivity metrics. Without structured data, organizations struggle to make the case for funding or measure progress against goals.
HealthFront Ventures' HealthFront Baseline™ is an AI-native HCP workforce data solution built for rural healthcare organizations. It delivers four quantitative metrics plus one rural county quality measure — establishing the baselines required to document gaps, measure progress, and support retention and recruitment funding applications under the RHT Program.
Launching Q1 2026 with FY25 baseline data, HealthFront Baseline™ focuses on tracking the measurable rural healthcare provider workforce: MDs and NPs/PAs.
Compounding Workforce Risk
That data infrastructure need is growing more urgent. Medicaid reductions projected to cause $8 billion in Oklahoma hospital losses over the next decade could accelerate provider departures from rural communities. Revenue losses force hospitals to cut services, reduce staff, and in extreme cases, close facilities entirely.
When rural hospitals close, providers lose practice settings and often relocate to urban areas. The RHT Program's workforce investments are a stabilization tool — but only if organizations can measure baselines, track retention, and demonstrate impact through quantitative data.
How Rural Healthcare Organizations Can Prepare and Participate
Monitor Official Program Channels
Check the official RHT Program website regularly for:
- New NOFO releases
- Public engagement meeting announcements
- Program updates and quarterly reports
- FAQ documents and webinar recordings
Sign up for OSDH email alerts and listservs to receive notifications immediately when new funding opportunities open.
Review the Initiative Funding Summary
Download the RHTP Initiative Funding Summary Packet and identify which of the 29 programs align with your organization's services. Cross-reference your capabilities against program goals to prioritize applications.
Attend Listening Sessions and Public Engagement Meetings
OSDH holds ongoing listening sessions and public engagement meetings across the state. Upcoming events include:
- RHTP Roadshows in Woodward (April 15), Chickasha (April 16), Muskogee (June 10), and Perry (June 18, 2026)
- Virtual RHTP Touchpoint Webinars on April 21 and June 17, 2026
Attending these sessions helps organizations understand upcoming funding priorities, provide community input that shapes program design, and network with state administrators and peer organizations.
Once you have a clear picture of relevant funding opportunities, the next priority is getting your administrative house in order before any application window opens.
Ensure Federal Registration Compliance
Before applying for any RHT funding, verify that your organization has:
- Active Unique Entity Identifier (UEI) registered at SAM.gov
- Current SAM.gov registration maintained throughout application, review, and award periods
- Certificate of Insurance meeting federal requirements
- No suspension or debarment on federal exclusion lists
SAM.gov registration can take weeks to process, so start early.
Document Rural Service Delivery
Prepare documentation demonstrating how your organization serves rural beneficiaries:
- Service area maps showing rural counties served
- Patient demographic data by county
- Partnership agreements with rural community organizations
- Examples of rural-specific programs or outreach
Even if headquartered in an urban area, documented rural engagement strengthens your application.
Establish Quantitative Workforce and Health Outcome Baselines
Organizations planning to apply for workforce-related initiatives will benefit from structured data on:
- Current provider counts by credential type (MD, NP, PA)
- Retention rates and turnover metrics
- Geographic coverage gaps and service area maps
- Provider productivity and panel sizes
Building this data infrastructure from scratch requires real IT investment and time. HealthFront Baseline™ offers a purpose-built alternative — four quantitative workforce metrics plus one rural county quality measure — giving organizations audit-ready baselines to demonstrate need, track progress, and report outcomes across CMS-aligned RHT initiatives.
Frequently Asked Questions
Who is eligible to apply for Oklahoma RHT Program funding?
Eligible entities include nonprofits, independent healthcare practices, community organizations, local governments, tribal governments, and partner state agencies operating in rural Oklahoma counties (population under ~50,000 outside Oklahoma and Tulsa counties). Specific requirements vary by individual NOFO; check each funding opportunity for detailed eligibility criteria.
How does Oklahoma define "rural" for the RHT Program?
Oklahoma defines rural as communities under approximately 50,000 residents not located in Oklahoma County or Tulsa County. This population-based definition covers approximately 75 of the state's 77 counties — a broader standard than HRSA's traditional rural classifications.
What is the total amount of funding Oklahoma received, and for how long?
Oklahoma received $223,476,948.62 for Budget Period 1 of a five-year cooperative agreement running through 2030. Additional funding is expected in subsequent budget periods pending CMS review and approval, with the national program distributing $10 billion annually across all 50 states.
What can RHT Program funds NOT be used for?
Funds cannot cover:
- Everyday operational expenses or services already funded by other federal programs
- Major renovations, staffing expenses, or student loan repayment (microgrant restrictions)
- New construction, broadband infrastructure, or ongoing subscriptions
- Food items or lobbying activities
Each NOFO details the full list of eligible and ineligible uses for that specific opportunity.
How does the Rural Health Transformation Program relate to Medicaid cuts?
The RHT Program was authorized alongside an estimated $911 billion in federal Medicaid reductions over a decade. State officials clarify its purpose is not to offset those cuts but to fundamentally transform rural care delivery — through workforce development, telehealth expansion, and value-based care models.
How will Oklahoma report on RHT Program outcomes?
Oklahoma produces quarterly and annual progress reports to CMS as part of the cooperative agreement structure, with monthly coordination calls with CMS officers. The OSDH continues to update the public through the RHT Program website, public engagement meetings, and webinars throughout the five-year funding period.


