Introduction
Roughly one-third of Oregonians live in rural or frontier communities, yet access to quality healthcare remains deeply unequal. Recent federal Medicaid cuts threaten to widen that gap significantly over the next decade. According to the Commonwealth Fund, more than 200 rural hospitals nationwide have closed or partially closed since 2005, with over 400 at risk.
Oregon's $197.3 million award under the federal Rural Health Transformation Program addresses that pressure directly — but understanding how it works matters as much as the dollar figure itself. This guide explains what the program is, how funding flows, and what it means for rural providers and communities. It covers:
- The program's origins and federal framework
- Oregon's five funding initiatives
- Award tiers and the application process
- The workforce dimension
- An honest look at the program's limitations
Key Takeaways
- H.R. 1 created the RHTP — a $50 billion federal program to offset Medicaid cuts and support rural healthcare from 2026–2031
- Oregon was awarded $197.3 million for 2026, with potential for more in later years based on performance
- Five initiatives — partnerships, prevention, workforce, technology, and a dedicated Tribal track — define what Oregon can fund
- Catalyst Awards (deadline: May 26) distribute ~$80M/year — the primary application pathway for eligible organizations
- $197M won't close the gap — rural Oregon faces $4+ billion in projected losses over the decade
What Is the Rural Health Transformation Program (RHTP) and Why Does It Exist?
The RHTP was established under Section 71401 of H.R. 1 (the "One Big Beautiful Bill Act"), the federal budget reconciliation law enacted in July 2025. The program is administered by CMS and distributes $50 billion across all 50 states between 2026 and 2031.
National Context for Rural Healthcare Crisis
The program's explicit purpose is offsetting damage to rural healthcare systems expected from Medicaid spending cuts embedded in the same legislation. Research shows that 24% of people in rural areas rely on Medicaid coverage, a higher share than in urban areas.
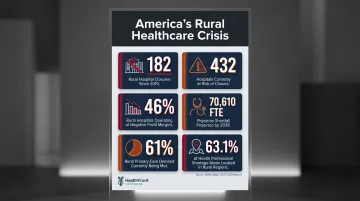
The underlying numbers tell a stark story. According to Chartis's 2025 analysis and HRSA's 2025 Primary Care Workforce report:
- 182 rural hospitals have closed or converted to no-inpatient models since 2010
- 432 rural hospitals are currently vulnerable to closure
- Nearly 46% of rural hospitals operate with negative margins
- A national primary care physician shortfall of 70,610 FTEs is projected by 2038
- Nonmetro areas are expected to meet only 61% of primary care demand by that date
- 63.1% of primary care Health Professional Shortage Areas (HPSAs) are in rural areas (as of December 2025)
Hospital closures feed the workforce gap directly — fewer facilities mean fewer practice sites, which accelerates provider departures from rural communities already struggling to recruit.
How Oregon's Allocation Was Determined
State allocations were determined through a weighted formula: 50% distributed equally across approved states, and 50% weighted by rural population size, proportion of rural healthcare facilities, and related CMS-defined factors. Annual awards are subject to federal review of each state's progress.
Oregon's allocation broke down as follows:
- Requested: $200 million per year ($1 billion over five years)
- Awarded for 2026: $197.3 million
- Future years: Contingent on demonstrated results from prior-year performance
The state will scale its plans to fit the available budget each cycle.
How Oregon's $197.3 Million Is Being Allocated
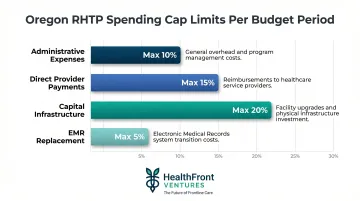
Oregon's allocation follows a structured approach with specific spending caps:
Spending Caps:
- Administrative expenses: Maximum 10% per budget period
- Direct provider payments: Maximum 15% of total award
- Capital infrastructure: Maximum 20% per period
- EMR replacement: Maximum 5% (if a certified EMR existed as of September 1, 2025)
Immediate Impact Awards
Approximately $6.5 million is directed to 12 pre-selected strategic projects that can launch within two months of receiving funding. These cover healthcare professional training, mental health and substance use prevention, and chronic disease management support.
Catalyst Awards: The Primary Competitive Pool
OHA expects to grant approximately $80 million per year for up to two years to ready-to-go projects in priority focus areas. The current application window closes May 26, and organizations must demonstrate they can launch within two months of receiving funding.
Tribal Initiative
A dedicated Tribal initiative flows directly to Oregon's nine federally recognized tribes to improve healthcare access and outcomes. Structured around the government-to-government relationship, this funding runs outside the competitive grant process entirely.
Sustainability & Infrastructure Funding (Later Years)
Later program phases will shift toward building durable capacity across Oregon's rural health system. Competitive funding in these years will target:
- Long-term sustainability of rural healthcare operations
- Shared infrastructure across provider networks
- Cross-sector collaboration between health, housing, and social services
OHA has committed to regular community engagement and federal reporting throughout the program lifecycle.
Oregon's Five Strategic Initiatives Under the RHTP
OHA's five-initiative framework organizes all non-tribal, non-administrative RHTP spending. These were developed through statewide community engagement prior to the federal application.
Healthy Communities & Prevention
This initiative expands preventive care reach, boosts chronic disease management programs, and improves maternal and child health outcomes. The four Catalyst Award priority areas are:
- Maternal and child health
- Co-occurring behavioral health conditions
- Aging in place
- Chronic disease management
Projects must be ready to launch within two months of receiving a Catalyst Award and must address measurable outcomes rather than infrastructure-only investments.
Workforce Capacity & Resilience
Oregon faces severe rural provider shortages. Oregon Office of Rural Health data shows 65 primary care HPSA-designated rural service areas across 28 counties. Statewide, Oregon has 117.1 primary care physicians per 100,000 population, but rural areas fall far below this average.
To address these gaps, this initiative funds:
- Recruitment and retention programs
- Healthcare professional training pipelines
- Expansion of NP/PA and community health worker workforce

Workforce investments require measurable outcome tracking. Organizations applying in this category need systems to document hiring rates, retention trends, and provider-to-population ratios over time — a requirement that purpose-built workforce data infrastructure, such as HealthFront Baseline™ (launching Q1 2026), is specifically designed to meet.
Technology & Data Modernization
This initiative improves health information technology, EHR adoption, telehealth infrastructure, and data systems in rural hospitals and clinics. CMS-approved uses include implementing new technologies and expanding data capabilities that support better care coordination and clinical decision-making.
Eligible technology investments include:
- EHR implementation and interoperability upgrades
- Telehealth platform expansion and broadband-dependent infrastructure
- Data systems supporting care coordination and population health reporting
Regional Partnerships & System Transformation
This initiative supports collaborative care delivery models, value-based arrangements, alternative payment structures, and hub-and-spoke networks that allow rural providers to share resources and specialty access across regions.
How to Apply: Catalyst Awards and Eligibility
Oregon's RHTP Catalyst Awards are open to a broad range of rural-serving organizations. Eligible applicants include:
- Local governments
- Rural hospitals and clinics
- Health systems
- Federally Qualified Health Centers (FQHCs)
- Behavioral health organizations
- Tribal health programs
- Community-based organizations operating in Oregon's rural and frontier communities
OHA defines "rural" as living at least 10 miles from a population center of 40,000 or more.
Catalyst Award Application Requirements
Proposals must:
- Address at least one of the four priority areas (maternal and child health, behavioral health, aging in place, chronic disease)
- Demonstrate readiness to launch within two months of award
- Align with Oregon's five strategic initiatives (detailed in OHA's official guidance documents at the application portal)
Application deadline: May 26, 2026
Where to Apply: Visit OHA's Rural Health Transformation Program webpage for official application materials (solicitation number S-44300-00016498), email update signups, and guidance documents.
Advisory Resources
Navigating the application process doesn't have to be done alone. The Rural Health Coordinating Council at OHSU's Oregon Office of Rural Health advises the Oregon RHTP and is a resource for organizations working through eligibility and planning questions. The council actively guides RHTP regional convenings and implementation planning.
The Workforce Imperative: What RHTP Means for Rural Healthcare Providers
Oregon's rural healthcare workforce crisis predates the RHTP. National data shows that 7.2% of U.S. counties had zero primary care physicians in 2023, and more than 35% of PCPs are 55 or older, signaling a wave of impending retirements.
RHTP funding creates a concrete opportunity for rural organizations to build or expand structured workforce retention and recruitment programs, including:
- Incentive planning
- Loan repayment support
- NP/PA pipeline development
- Partnership with training institutions
The Accountability Challenge
Accessing this funding requires demonstrating that programs are tied to measurable outcomes. Workforce accountability under the RHTP means organizations will need reliable baseline data on provider counts, vacancy rates, and turnover by county or region.
That data infrastructure is where many rural organizations hit a wall — building it from scratch takes time and capacity that most don't have.
HealthFront Ventures' HealthFront Baseline™ (launching Q1 2026) addresses this directly. The outsourced service tracks rural HCP workforce metrics — four quantitative measures plus one rural county quality measure — without requiring custom-built solutions. It's designed to align with federal reporting requirements at a time when organizational bandwidth is already stretched thin.
The Funding Gap: Limitations and Long-Term Sustainability
The Adequacy Problem
KFF analysis estimates $137 billion in Medicaid reductions over 10 years in rural areas nationally. Oregon's $197.3 million first-year RHTP award covers only a fraction of projected losses.
As OHA Health Policy & Analytics Director Clare Pierce-Wrobel stated: "This much-needed boost can't make up for the substantial federal funding cuts we anticipate."
Per-Capita Disparities
Per-rural-resident RHTP allocations vary sharply across states:
| State | Per Rural Resident Award |
|---|---|
| Rhode Island | $6,305 |
| Texas | $66 |
The allocation formula weights rural population size, proportion of rural facilities, and hospital status — factors that heavily favor smaller, more rural states over large ones.
The Five-Year Sunset
RHTP funding ends in 2031. Rural organizations and state planners must design programs that either:
- Become self-sustaining through value-based payment models
- Align with other funding streams
- Demonstrate sufficient outcomes to justify state-level funding continuation

Build infrastructure, not subsidies. One-time investments in data systems, workforce pipelines, and telehealth capacity outlast the funding window. Ongoing service subsidies will need replacement funding after 2031 — infrastructure investments won't.
That distinction shapes how Oregon's awardees should allocate dollars now, while the window is open.
Frequently Asked Questions
What is the Oregon Rural Health Transformation Program (Section 71401)?
The Oregon RHTP is the state's implementation of the federal Rural Health Transformation Program established under Section 71401 of H.R. 1, funded by CMS, awarding Oregon $197.3 million in 2026 to improve rural healthcare access, workforce, and infrastructure.
Who is eligible to apply for the Oregon Rural Health Transformation Program?
Eligible applicants include rural hospitals, clinics, local governments, community-based organizations, FQHCs, behavioral health providers, and tribal health programs operating in Oregon's rural and frontier areas. Check OHA's program webpage for eligibility details.
What are the four priority areas for Catalyst Award funding?
The four priority areas are maternal and child health, co-occurring behavioral health conditions, aging in place, and chronic disease management. Applicants must address at least one of these areas in their project proposal.
How much total funding is available through the Catalyst Awards?
OHA expects to award approximately $80 million per year for up to two years through Catalyst Awards, drawn from the roughly $157 million available after the Tribal Initiative and administrative allocations are set aside.
Will RHTP funding make up for Oregon's Medicaid cuts?
No. The $197.3 million award covers only a fraction of the billions in Medicaid funding rural Oregon is projected to lose over the next decade. The program supports transformation and innovation — it is not a substitute for lost coverage funding.
When is the Catalyst Award application deadline?
The current Catalyst Award application window closes May 26, 2026. Visit OHA's Rural Health Transformation Program webpage for application materials and to sign up for updates on future funding rounds.