This is the daily reality for thousands of Neighbor Island residents. Hawaii may conjure images of world-class resorts and pristine beaches, but for the 593,603 people living in rural areas across Maui, Molokaʻi, Lanaʻi, and the Big Island, accessing basic healthcare often means traveling hours across water. The state's only Level 1 trauma center sits in Honolulu. Behavioral health specialists are scarce. Digital health infrastructure is fragmented.
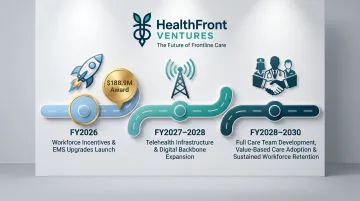
The $188.9M federal award Hawaii just received from the Centers for Medicare & Medicaid Services (CMS) is designed to close this gap. This article explains what the Hawaii Rural Health Transformation Program (RHTP) is, why it matters, the six funded initiatives it supports, and what rural providers and communities can expect over the next five years.
TLDR: Key Takeaways
- Hawaii received $188,892,440 for FY2026 under CMS's $50 billion national Rural Health Transformation Program, with annual awards expected through 2030
- Six initiatives cover digital infrastructure, telehealth, emergency services, behavioral health, workforce development, and value-based care
- 95%+ of Hawaii's land is rural, but care remains concentrated on Oʻahu — a gap this funding directly targets
- HOME RUN builds a "grow your own" provider pipeline — scholarships, residencies, and mentoring designed to keep rural clinicians in rural communities
The Rural Healthcare Crisis That Made This Funding Necessary
Hawaii's rural health challenge is unique. While the state is geographically compact, its island geography creates barriers no mainland rural community faces. You can't drive to the next county for care. Inter-island travel is expensive, unreliable, and time-consuming.
Those barriers show up in the data:
- 95.1% of Hawaii's land area is federally classified as rural
- 40.8% of residents (593,603 people) live in rural areas
- Healthcare services are heavily concentrated on Oʻahu
Research from the University of Hawaii's Rural Health Research and Policy Center documented frequent flight delays and cancellations affecting Molokaʻi and Lanaʻi residents — forcing multi-month rescheduling for high-need care.
The financial toll compounds the problem. A University of Iowa policy analyst specializing in Hawaii detailed typical costs: $120 round-trip airfare plus $40–50 in ground transport, often aboard small planes prone to weather delays.
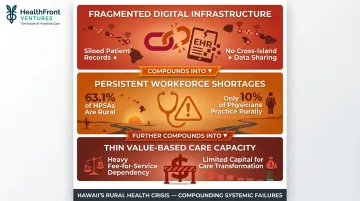
Three Systemic Failures
Beyond geography, three systemic problems compound Hawaii's rural health crisis:
- Fragmented digital infrastructure: Rural hospitals and clinics operate with siloed EHRs and limited data interoperability. When a patient travels from Molokaʻi to Honolulu for specialty care, critical health records often don't follow them.
- Persistent workforce shortages: 63.1% of designated primary care Health Professional Shortage Areas (HPSAs) are in rural areas, yet only about 10% of U.S. physicians practice rurally. Molokaʻi — population ~7,400, 65% Native Hawaiian — has no on-island specialists, surgery capabilities, or anesthesia services.
- Thin value-based care capacity: Transitioning from fee-for-service to value-based models requires capital and technical infrastructure most rural facilities don't have.
These failures — documented through data, fieldwork, and community testimony — made the case for federal intervention. In July 2025, Hawaii launched a formal rural health planning process incorporating healthcare leader meetings and the Engage Hawaiʻi public feedback platform. That community-driven process shaped the transformation plan ultimately submitted to CMS.
What Is the Hawaii Rural Health Transformation Program?
The Hawaii RHTP is a five-year cooperative agreement funded by CMS under the $50 billion national Rural Health Transformation Program established through H.R. 1 (Public Law 119-21).
How the funding works:
- Hawaii's award: $188,892,440 for FY2026
- Additional annual funding expected through FY2030
- Funding is performance-based and contingent on state outcomes
CMS distributes roughly $10 billion annually across all 50 states. Individual state awards in FY2026 ranged from approximately $147 million to $281 million. That allocation uses a hybrid formula: 50% divided equally among approved states, and 50% based on rural population and health system metrics.
Governance and Accountability
CMS releases funds to Hawaii's Governor's Office under a cooperative agreement, which then issues subawards to initiative leads:
- State Health Planning and Development Agency (SHPDA)
- University of Hawaii's Telecommunication and Social Informatics Program (TASI)
- UH John A. Burns School of Medicine (JABSOM)
- Hawaii Department of Health
- Hawaii Department of Human Services
Accountability runs through CMS's newly created Office of Rural Health Transformation, led by director Alina Czekai. Hawaii must submit quarterly and annual reports covering both spending and outcomes. Performance metrics are geographically specific — ensuring resources reach the most underserved rural areas rather than concentrating near population centers.
On a per-rural-resident basis, Hawaii's award translates to approximately $318 per rural resident — one of the highest per-capita figures nationally. That rate reflects the real cost of delivering care across six inhabited islands with dispersed rural populations and no overland infrastructure connecting them.
Breaking Down Hawaii's Six RHTP Initiatives
Hawaii's transformation plan centers on six interconnected initiatives addressing complementary gaps in rural healthcare infrastructure and delivery.
Digital Infrastructure and Virtual Care
Initiative 1: Rural Health Information Network (RHIN)
RHIN creates a statewide shared data network linking rural hospitals, clinics, and health centers through interoperable electronic health records, secure wireless networks, referral systems, and shared data hubs.
In practice: When a patient moves between rural clinics and urban specialists, critical health information often doesn't follow. RHIN solves this fragmentation, enabling seamless care coordination across islands.
Initiative 2: Pili Ola Telehealth Network
This statewide system connects rural communities to providers through virtual care platforms and expands telehealth training programs.
For rural patients: Behavioral health access is especially limited in rural Hawaii. Telehealth enables rural residents to access psychiatrists, psychologists, and counselors without traveling to Honolulu.
Care Access and Behavioral Health
Initiative 3: Rural Infrastructure for Care Access (RICA)
RICA expands emergency medical services (EMS), deploys mobile healthcare units, launches community paramedicine programs, and builds behavioral health capacity in rural areas.
Community paramedicine is particularly relevant for Hawaii's island geography. Rather than traditional emergency-only EMS, community paramedics provide ongoing care for chronic conditions, post-discharge follow-up, and preventive services in patients' homes. Research shows Mobile Integrated Health/Community Paramedicine programs reduce emergency department visits by approximately 44%.
The impact: When EMS response times are measured in inter-island transfers rather than minutes, community paramedicine can prevent avoidable emergencies and hospitalizations.
Initiative 4: Details on this initiative are not yet publicly available in program documentation.
Initiative 5: Rural Respite Network (RRN)
RRN expands the medical respite model to rural areas, providing short-term residential care for unhoused individuals and post-acute patients with low medical acuity who don't need hospital-level care but aren't healthy enough to recover on the streets or in shelters.
A cohort study of medical respite programs found significantly reduced inpatient utilization compared to usual care. By preventing avoidable hospitalizations, medical respite addresses an often-overlooked driver of rural emergency department overutilization.
Care Model Innovation
Initiative 6: Rural Value-Based Innovation (RVBI) and AHEAD Readiness Fund
This competitive fund enables rural providers to adopt innovative care models and prepare for CMS's Achieving Healthcare Efficiency through Accountable Design (AHEAD) payment model.
AHEAD is a voluntary state-based model designed to improve quality and lower total cost of care. Its core components include:
- Global hospital budgets that shift reimbursement away from volume-based fee-for-service
- Enhanced primary care payments to strengthen preventive and coordinated care
- Quality performance targets tied to population health outcomes
Most rural providers can't transition away from fee-for-service due to limited capital and technical capacity. This fund addresses that barrier directly.

Workforce Pipeline: HOME RUN and the Rural Provider Retention Challenge
Initiative 4—HOME RUN (Hawaiʻi Outreach for Medical Education in Rural Under-resourced Neighborhoods)—tackles one of rural healthcare's most persistent challenges: recruiting and retaining qualified providers.
Why "Grow Your Own" Works
HOME RUN uses scholarships, rural residency programs, certificate training, and structured mentoring to build a homegrown rural healthcare workforce.
Evidence shows this approach works. Research summarized by the National Rural Health Association demonstrates that:
- Clinicians with rural backgrounds are more than twice as likely to remain in rural practice
- Rural residencies make physicians 2-3 times more likely to practice rurally long-term
- Non-clinical factors like spousal employment, childcare, and affordable housing are decisive retention drivers
HOME RUN targets all these factors: recruiting trainees from Neighbor Island communities, providing residency experiences in rural settings, and offering financial incentives that address cost-of-living barriers.
The Data Challenge
Rural organizations participating in RHTP must establish baseline workforce metrics—provider counts, vacancy rates, turnover rates—to document need and demonstrate improvement over the program's five-year period.
That's where HealthFront Baseline™ fits in. HealthFront Ventures provides AI-native workforce data infrastructure with quantitative metrics designed specifically for rural healthcare provider tracking (MDs and NPs/PAs).
Launching in Q1 2026 with FY25 baseline data, HealthFront Baseline™ gives rural health organizations a measurable starting point and ongoing performance tracking aligned with RHTP accountability requirements. Organizations get purpose-built data infrastructure without having to build it themselves.
Timeline and Early Wins
State officials indicated that some improvements could move quickly once funds are released, while others will take longer:
- Near-term: Workforce incentives and EMS upgrades are expected to roll out relatively soon after funding is available
- Longer-term: Statewide telehealth expansion and value-based care team development require more time to implement
For organizations aiming to document pre-program conditions, workforce baseline measurement needs to happen before interventions begin.
Funding Flow, Oversight, and Implementation Timeline
How the Money Moves
CMS releases funds to Hawaii's Governor's Office under a cooperative agreement structure. The Governor's Office then issues subawards to initiative leads—state agencies and University of Hawaii entities. States cannot unilaterally decide allocation. CMS retains final authority through its Office of Rural Health Transformation, reviewing how funds are distributed across all six initiatives.
As of the January 2026 announcement, approved uses of funds were still under review. Final allocation across all six initiatives remained under negotiation with CMS.
Key structural guardrails include:
- CMS cooperative agreement approval required before subawards issue
- University of Hawaii entities designated as eligible initiative leads
- Final allocation subject to CMS sign-off, not state discretion alone
The Reporting and Performance Cycle
Quarterly and annual reporting requirements:
- Both spending and outcome metrics must be reported
- First-year reporting begins mid-2026
- Next fiscal year spending begins October 2026
Those metrics aren't just aggregate numbers — they're geographically specific. That design choice ensures funding reaches the most underserved rural areas rather than concentrating near Honolulu or other population centers.
The Five-Year Arc
FY2026 represents year one of a five-year program. Continued annual awards through 2030 are contingent on demonstrated state performance. Year-one priorities focus on emergency response and mental healthcare capacity, with workforce and digital infrastructure scaling through 2030.
Program milestones by fiscal year:
- 2026: Workforce incentive programs and EMS upgrades launch
- 2027-2028: Telehealth infrastructure expansion and digital backbone buildout
- 2028-2030: Full care team development, value-based care model adoption, and sustained workforce retention outcomes
Frequently Asked Questions
What is the Hawaii Rural Health Transformation Program?
The Hawaii RHTP is a five-year, CMS-funded initiative providing Hawaii with $188.9M in FY2026 as part of a $50B national program. It aims to improve healthcare access, infrastructure, and workforce in rural and Neighbor Island communities, with annual funding expected through 2030.
Who is eligible to apply for the Hawaii Rural Health Transformation Program?
RHTP is a state-administered cooperative agreement—Hawaii's Governor's Office receives and distributes funds to designated initiative leads and subawardees, including state agencies and University of Hawaii entities. Rural healthcare providers should monitor the Governor's Office and participating subawardees for contract and grant opportunities.
What is the 1.5 medical rule in Hawaii?
The "1.5 medical rule" is not a clinical practice or provider licensing regulation in Hawaii. The closest match is a financing provision in the Hawaii Prepaid Health Care Act: employee premium contributions cannot exceed 1.5% of monthly wages. This is an employer insurance contribution cap, not a medical practice rule.
How is Hawaii's $188.9M RHTP funding being distributed among the six initiatives?
The final allocation across the six initiatives is determined through negotiation between Hawaii's Governor's Office and CMS under the cooperative agreement structure. Specific per-initiative dollar amounts were not publicly confirmed at the time of the initial award announcement.
When will Hawaii residents start seeing results from the Rural Health Transformation Program?
Workforce incentive programs and EMS upgrades are expected to launch relatively quickly once funding is released. Telehealth infrastructure and care team development will take longer, with the most significant systemic improvements projected over the full five-year period through 2030.
How does Hawaii's RHTP award compare to other states nationally?
While the $188.9M award falls within the national range (approximately $147M to $281M per state in FY2026), Hawaii's award is notable on a per-rural-resident basis. At roughly $318 per rural resident, it ranks among the highest per-capita investments in the country—driven largely by Hawaii's geographic isolation and multi-island delivery challenges.
Hawaii's $188.9M RHTP is the largest rural health investment in the state's history. For Neighbor Island communities facing persistent gaps in specialty care, behavioral health, and workforce stability, it offers a concrete path forward. Whether that potential is realized depends on execution: deploying the infrastructure, building the workforce pipelines, and tracking outcomes that prove sustained improvement through 2030.