KFF projects that rural South Dakota faces approximately $487 million in federal Medicaid spending reductions over the next decade, with an estimated 13,000 residents losing coverage due to new work requirements. The RHTP exists as a direct congressional response to this anticipated harm—a dedicated fund to protect rural providers from cuts that would otherwise threaten sustainability.
This article covers South Dakota's $189.4 million award, the 10 strategic initiatives funded through the program, the workforce-focused components, and the practical next steps rural healthcare organizations should take now.
TLDR: Key Takeaways
- The One Big Beautiful Bill Act created a $50 billion Rural Health Transformation Program (FY2026–2030)
- South Dakota received $189.4 million for 2026, versus the $193.3 million requested for year one
- Governor Rhoden signed HB 1044 on January 29, 2026, granting spending authority to the SD Department of Health
- SD's plan covers 10 initiatives, ranging from $3.5 million to $500 million per program area
- Rural healthcare organizations need current workforce baselines to qualify for incentive programs and track outcomes
What Is the South Dakota Rural Health Transformation Program?
Congress established the RHTP through Section 71401 of the One Big Beautiful Bill Act (H.R. 1, Public Law 119-21), signed into law by President Trump on July 4, 2025. The program was a direct legislative response to concerns that the bill's Medicaid provisions would harm rural healthcare providers, following KFF analysis projecting significant coverage losses and revenue reductions.
Rural South Dakota is projected to lose approximately $487 million in federal Medicaid spending over the next decade, driven by new work requirements (80 hours monthly by 2027) that could affect an estimated 13,000 South Dakotans. Twenty percent of South Dakota hospitals already operate at negative margins. The RHTP was designed to offset that fiscal pressure.
Program Structure
CMS administers $10 billion annually across all 50 states for five years (FY2026–2030). The allocation formula splits funding evenly:
- 50% distributed equally among all approved states that submitted qualifying applications
- 50% awarded competitively based on rural population share, number of rural facilities, and hospital stress factors
States must propose uses in at least three of the five allowable strategy domains and demonstrate coordinated planning involving health systems, provider associations, tribal nations, and community stakeholders.
Five National Strategic Goals
| Strategic Goal | Description |
|---|---|
| Make rural America healthy again | Preventive health innovations, chronic disease management, behavioral health, prenatal care |
| Sustainable access | Helping rural providers become long-term access points through efficiency and regional coordination |
| Workforce development | Recruitment and retention of providers, including community health workers and pharmacists, practicing at top of license |
| Innovative care models | New care models and payment mechanisms incentivizing lower costs and improved quality |
| Technology and innovation | Digital health tools, remote care, data sharing, and cybersecurity |

The NOFO was released September 15, 2025, with applications due November 5, 2025 and awards announced December 29, 2025. States are now in the execution phase — the focus has shifted from who applied to how funding gets deployed on the ground.
South Dakota's $189.4 Million Award: Key Details
CMS announced South Dakota's FY2026 award of $189,477,607.26 on December 29, 2025. The state requested $193.3 million for year one and approximately $1 billion over five years—meaning the FY2026 allocation came in approximately $4 million short of the request. Award amounts can change annually based on congressional appropriations and program performance.
Collaborative Application Process
South Dakota's application involved extensive collaboration among state agencies, health systems, tribal partners, and provider organizations:
- State agencies: SD Department of Health (DOH), SD Department of Social Services, Bureau of Information and Telecommunications
- Major hospital systems: Avera Health, Sanford Health, Monument Health
- Tribal partners: Great Plains Tribal Leaders Health Board, Indian Health Service, nine federally recognized tribes
- Provider associations: South Dakota Association of Healthcare Organizations (SDAHO)
- Community health centers: Complete Health, Falls Community Health, Horizon Health Care, Rural Health Care
- Educational institutions: Lake Area Technical College, Southeast Technical College, state universities and medical schools
Health Secretary Melissa Magstadt emphasized the community-centered design: "The Rural Health Transformation initiative drives stronger, more integrated and connected health care systems to meet people where they are."
Legislative Authorization
Governor Larry Rhoden signed HB 1044 on January 29, 2026—not February as sometimes reported—granting the SD Department of Health spending authority to execute the RHTP. The bill passed the House 56-11 and the Senate 32-2, reflecting strong bipartisan support. Governor Rhoden called it "the most significant investment in rural healthcare in South Dakota's history."
Regional Comparison: Neighboring State Awards
| State | FY2026 Award | Comparison to Request |
|---|---|---|
| South Dakota | $189.4 million | Below request (~$4M short) |
| Montana | $233 million | — |
| Nebraska | $218.5 million | 8th-highest nationally |
| Iowa | $209 million | Above request |
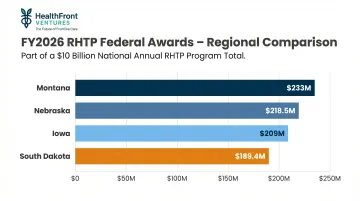
South Dakota received the lowest FY2026 award among these four neighbors. The allocation formula weights rural population size, facility counts, and measures of hospital financial distress—factors that pushed neighboring states with larger rural footprints to higher awards. For SD planners, the ~$4 million gap relative to the request is a real constraint worth building into multi-year budget projections.
Understanding the Medicaid Offset
The One Big Beautiful Bill Act's Medicaid provisions are projected to reduce rural coverage and provider revenue during the same period the RHTP operates. That timing matters: rural healthcare organizations should plan for simultaneous RHTP investment and Medicaid contraction. In practice, transformation funds may partially offset revenue losses rather than representing net-new expansion capital.
Strategic Focus Areas: Where the $189.4 Million Goes
South Dakota's approved application includes 10 initiatives organized around four major focus areas. The initiatives range from $3.5 million to $500 million over five years.
Connecting Technology and Data
Tech and Data Connection for a Healthier South Dakota ($500 million, five-year total)
This flagship initiative creates the **South Dakota Health Data Atlas**, a centralized platform allowing health systems statewide to share and access health data in one unified system. The initiative operates through three tiers:
- Tier 1: EHR implementation and training for small practices and Tribal clinics
- Tier 2: Advanced integration (interoperability, telehealth, population health tools) for mid-size facilities
- Tier 3: Regional Innovation Hubs where large systems mentor smaller facilities
The initiative also covers a broad infrastructure layer, including:
- Telecommunications upgrades and certified EHR systems
- ePrescribing and AI-powered clinical decision support
- Robotic surgical and diagnostic systems
- Cybersecurity measures (encryption, multi-factor authentication)
- Backup power systems and emergency generators
Advancing the Rural Workforce
Filling provider gaps requires more than technology — it demands sustained investment in the people delivering care. Three initiatives target this directly:
Building a Sustainable Rural Healthcare Workforce — Led by the SD Office of Rural Health and Emergency Services, this initiative combines recruitment incentives (sign-on bonuses, relocation assistance, rural service stipends) with education supports (tuition assistance, paid clinical release time, flexible training pathways). Workforce funding recipients must commit to a minimum five years of rural service.
Expand and Strengthen Rural Community Health Worker Workforce ($3.5 million) — The smallest initiative by dollar amount targets care coordination, health education, and patient navigation gaps in rural and frontier counties by building out the community health worker pipeline.
Rural Health Forward: Training and Resource Hub — A centralized hub providing educational resources, best practice sharing, and professional development for rural healthcare teams statewide.
Keeping Healthcare Local and Strong
Medicaid Rural Health Access and Quality Grants ($125 million) — Direct sustainability grants to rural providers facing operational pressure, designed to preserve local access points and prevent facility closures.
Beyond financial sustainability, four initiatives address specific care gaps:
- Chronic Disease Management: Programs targeting diabetes, hypertension, and cardiovascular disease — conditions that hit rural populations harder than urban ones
- Regional Maternal and Infant Health Hubs: Coordinated maternal services across rural regions, responding to the fact that 38 of South Dakota's 66 counties are classified as maternity care deserts
- Integrated Behavioral Health (CCBHC & Collaborative Care): Expansion of Certified Community Behavioral Health Clinics with collaborative care models embedding behavioral health directly into primary care
- Enhancing Sustainable EMS: Infrastructure, equipment, and staffing support for rural emergency medical services — a persistent vulnerability in frontier counties
Transforming Systems for Sustainability
Medicaid Primary Accountable Care Transformation (PACT)
New Medicaid payment models incentivizing coordinated care, cost control, and quality improvement through primary care-centered accountable care organizations.
The Workforce Initiative: A Closer Look
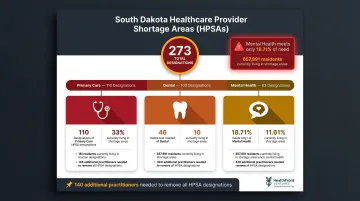
South Dakota carries 273 total Health Professional Shortage Area (HPSA) designations: 110 primary care, 100 dental, and 63 mental health. Mental health is the most severe shortage, meeting only 18.71% of need, with 657,991 people (approximately 72% of the state's population) living in mental health HPSAs. The state requires 140 additional practitioners to remove all shortage designations.
The workforce initiative operates through a two-pronged approach:
Recruitment Incentives
- Sign-on bonuses for providers committing to rural service
- Relocation assistance covering moving costs and temporary housing
- Rural service stipends providing ongoing financial support during the five-year commitment period
Education-Focused Supports
- Tuition assistance for students pursuing rural healthcare careers
- Paid clinical release time allowing practicing providers to pursue additional training without income loss
- Flexible training pathways accommodating the scheduling constraints of rural practice environments
Together, these create a pipeline from education into sustained rural practice—addressing both the shortage of new providers entering rural communities and the retention challenge once they arrive. Measuring whether that pipeline is working, however, depends entirely on having something to measure against.
Why Baseline Workforce Data Matters
To track progress over the five-year program, participating organizations need documented starting points for key workforce metrics:
- Provider vacancy rates by specialty and facility type
- NP/PA fill rates compared to authorized positions
- Retention rates measured at 1-year, 3-year, and 5-year intervals
- Time-to-fill for open provider positions
- Geographic distribution of providers across frontier vs. rural counties
Most rural organizations don't have these figures readily documented. Organizations that establish a clear baseline now — headcount, vacancy, and retention by specialty — will be better positioned to apply for incentive programs, demonstrate measured need, and report outcomes against RHTP requirements.
HealthFront Ventures' HealthFront Baseline™, launching Q1 2026, is designed specifically for this purpose. It tracks four quantitative workforce measures plus one rural county quality measure, giving organizations an outsourced data infrastructure option rather than building internal tracking systems from scratch.
Implementation Timeline: Where Things Stand
Key Milestones
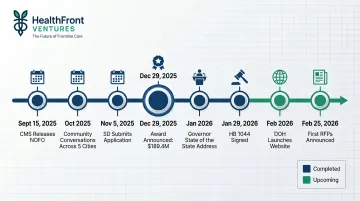
- September 15, 2025: CMS releases NOFO on grants.gov
- October 2025: Community conversations held in Yankton, Eagle Butte, Rapid City, Pierre, and Aberdeen (exact month not officially confirmed)
- November 5, 2025: South Dakota submits application
- December 29, 2025: CMS announces SD awarded $189.4 million
- January 2026: Governor Rhoden addresses program in State of the State
- January 29, 2026: HB 1044 signed into law, granting DOH spending authority
- February 2026: SD Department of Health begins sharing program details and launches ruralhealthtransformation.sd.gov with 10 initiative summaries
- February 25, 2026: First round of Requests for Proposals (RFPs) announced for leadership and project management roles
That community input phase mattered. Engagement sessions across five locations gathered public feedback that directly shaped South Dakota's application, reflecting a deliberate choice to build the program from local needs rather than a centralized template.
For the most current information on initiative rollout timelines, visit ruralhealthtransformation.sd.gov and monitor SDAHO member communications. New RFP announcements and initiative details are being added as each phase launches.
What Rural Healthcare Organizations Should Do Now
1. Review the 10 Initiative Summaries
Visit ruralhealthtransformation.sd.gov and review all 10 initiative summaries. Identify which initiatives align with your organization's service area, patient population, and workforce needs — this is the starting point for any meaningful RHTP participation.
2. Establish Current Workforce Data Baselines
Organizations that can document current provider headcount, vacancy, and retention figures today will be far better positioned to:
- Apply for workforce incentive programs with demonstrated need
- Measure outcomes against RHTP metrics over the five-year period
- Demonstrate program impact to state agencies and CMS
- Identify specific gaps and match them to appropriate initiative funding streams
Organizations without internal data warehouse capabilities may benefit from outsourced infrastructure built specifically for rural HCP workforce tracking. HealthFront Ventures offers AI-native data warehouses that capture the provider headcount, vacancy, and retention metrics RHTP programs require.
3. Engage with SDAHO and the 2026 Rural Health Leaders Conference
The 2026 Annual South Dakota Rural Health Leaders Conference is scheduled for June 24-25, 2026, at the Ramkota Hotel and Conference Center in Pierre, SD. The theme is "A Century Strong: Charting the Next Frontier of Rural Health." This conference serves as the state's primary channel for RHTP updates on program governance, funding distribution, and member-level participation opportunities.
Stay engaged with SDAHO communications as the association will continue to release guidance on how rural healthcare organizations can participate in specific initiatives as implementation details are finalized.
Frequently Asked Questions
What is the South Dakota Rural Health Transformation Program?
South Dakota's RHTP is a state-executed program funded under the federal One Big Beautiful Bill Act's $50 billion Rural Health Transformation Program. It aims to modernize rural healthcare delivery, workforce, and infrastructure from FY2026 through FY2030.
How much funding did South Dakota receive from the RHTP?
South Dakota was awarded $189.4 million for FY2026, slightly below the $193.3 million requested for year one. The state expects at least $500 million in total federal funding over five years, though annual allocations are not guaranteed.
Who benefits from South Dakota's RHTP funding?
The program benefits rural healthcare facilities, providers, and patients across South Dakota. While applications are submitted at the state level, funding flows through specific initiatives targeting workforce, infrastructure, chronic disease, behavioral health, and EMS programs in rural communities.
What is the "Building a Sustainable Rural Healthcare Workforce" initiative?
Led by the SD Office of Rural Health, this initiative uses recruitment incentives — sign-on bonuses, relocation assistance, and rural service stipends — alongside tuition assistance and flexible training programs. The goal is to attract and retain healthcare professionals in rural and frontier communities.
What is the South Dakota Health Data Atlas?
The Health Data Atlas is a proposed centralized platform under the $500 million technology and data infrastructure initiative. It would allow health systems statewide to share and access data in one unified system, with the broader initiative also covering telecom, equipment, emergency preparedness, and cybersecurity.
How does South Dakota's RHTP award compare to neighboring states?
Montana received $233 million, Nebraska $218.5 million, and Iowa $209 million for FY2026. South Dakota's $189.4 million award is the lowest among these four neighbors, though state officials still called it a significant outcome given South Dakota's rural population size and facility distribution.