
Introduction
Rural Americans face a compounding disadvantage that extends far beyond simple geography. They experience higher rates of preventable mortality, chronic disease, and uninsured status, all while navigating communities with limited healthcare access. According to CDC data, rural age-adjusted death rates were 20% higher than urban rates by 2019 — a dramatic widening from just 7% in 1999.
Accountable Care Organizations (ACOs) represent one of Medicare's flagship value-based care models, designed to coordinate care and improve quality while reducing costs. Rural ACOs, however, are structurally disadvantaged by design — they disproportionately serve patients with the greatest social needs, operate under benchmarking systems that penalize early efficiency gains, and contend with workforce shortages no reimbursement formula directly fixes.
This article examines ACOs' impact on rural health disparities, the structural and policy barriers standing in the way, and the data infrastructure investments rural organizations need to succeed in value-based care.
Key Takeaways
- ACOs coordinate care but lack an explicit mandate to reduce health disparities — any equity benefit is indirect
- Three or more consecutive years of ACO participation correlates with reduced rural health disparities, though no definitive causal link has been established
- Rural ACOs face unique barriers: workforce shortages, limited broadband, weak post-acute networks, and benchmarking that penalizes efficiency
- MSSP and ACO REACH reforms (2023) address some structural disadvantages, but community resource scarcity limits policy impact
- County-level baseline data on rural MD, NP, and PA supply is essential for ACO planning and execution
What Are ACOs and Why Do Rural Health Disparities Persist?
Accountable Care Organizations: A Brief Primer
Accountable Care Organizations are voluntary groups of doctors, hospitals, and other providers that coordinate high-quality care for their Medicare patients under programs like the Medicare Shared Savings Program (MSSP). When an ACO successfully improves quality while reducing spending below a regional benchmark, it earns a share of the savings.
The critical limitation: ACOs have no explicit mandate to reduce health disparities. Any equity benefit is a secondary, theoretically indirect result of better care coordination. This design gap creates real challenges for organizations serving rural and minority populations, where the highest social needs and thinnest community resources converge.
The Rural Health Disparity Landscape
The health outcome gap between rural and urban America is measurable, documented, and widening. Key disparities include:
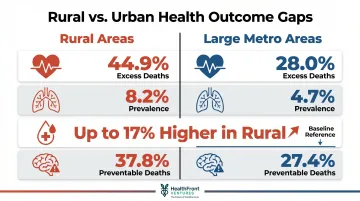
Preventable mortality and chronic disease:
- Heart disease potentially excess deaths: 44.9% in rural areas vs. 28.0% in large metro areas (2010–2017)
- COPD prevalence: 8.2% in rural adults vs. 4.7% in large metropolitan areas
- Diabetes prevalence: 9% to 17% higher in rural areas than urban areas, varying by state
- Stroke preventable deaths: 37.8% rural vs. 27.4% large metro
Coverage and access:
- Rural adults uninsured rate: 17.9% in 2020
- Higher poverty rates and older populations compound barriers to care
The Double Disadvantage
Minority populations in rural areas face compounding pressures: geographic isolation from care plus the racial and ethnic disparities that follow them regardless of location. Research on rural Latino Medicare beneficiaries illustrates this directly — diabetes-related hospitalization gaps between rural Latino and White older adults were significant even after controlling for income and coverage.
That gap points to a structural problem: ACOs operating in rural areas may improve average quality scores without moving the needle for the highest-need patients within those communities.
What the Research Reveals About ACOs and Rural Health Disparity Outcomes
Longitudinal Evidence From 516 Rural Health Clinics
A 2022 study published in Population Health Management tracked 516 rural health clinics in California, Florida, and Texas over eight years (2008–2015). Researchers found a statistically significant decrease in diabetes-related hospitalization disparities between rural Latino and White Medicare patients — a meaningful signal that conditions for rural minority patients were improving.
While disparity decreased over time, ACO participation alone was not a statistically significant causal factor. Continuous ACO participation over 3 consecutive years, however, showed moderate evidence of association with lower disparity (t = -1.947, p = 0.0525).
Key takeaway: Short-term or intermittent ACO participation appears insufficient to reduce health disparities in any measurable way.
The Time and Organizational Maturity Factor
Building the collaborative infrastructure ACOs need — clinical protocol alignment, staff training, community trust, and data systems — takes years before patient-level outcomes measurably improve. Prior research cited in the study confirms that early ACO benefits appear first as shared learning among member organizations, well before financial or health outcomes shift.
The policy implication is direct: expecting rural ACOs to demonstrate equity improvements within a 1-2 year performance measurement window sets an unrealistic bar. Rural ACOs need longer runway to show results.
What ACO Leaders Report About Social Risk
Qualitative research published in Health Affairs interviewed leaders of 49 MSSP ACOs and found:
- Most ACOs stratify patients by medical risk (claims-based) rather than social risk
- The most vulnerable rural patients — who have low healthcare utilization and thus few claims — are systematically missed by risk stratification tools built for more engaged patient populations
- Uncertainty about shared savings and tight margins hinder consistent social-needs investments
Despite these limitations, ACO social and clinical programs typically operate on a payer-agnostic basis, extending benefits to the broader patient population beyond just Medicare ACO members. Research shows that successful rural ACO investment in care coordination infrastructure could generate community-wide health improvement beyond what the data directly captures.
The Distinct Barriers Rural ACOs Face
Geographic and Infrastructure Barriers
The physical reality of rural care coordination differs from urban settings in ways that directly impair ACO performance:
- Travel distances: Patients must travel long distances for specialist visits, follow-up care, or post-acute services
- Broadband limitations: Rural older adults have significantly lower telehealth use than urban peers (incidence rate ratio 0.78, p<0.001), driven partly by limited broadband access
- Transportation deserts: No rideshare, limited public transit — care coordination plans that work in urban settings simply do not translate
- Weak post-acute networks: Rural ACOs typically have limited long-term care options, making it structurally difficult to build high-value care transitions

These geographic barriers directly impair core ACO functions required for shared savings performance.
Workforce Shortages and the NP/PA Pipeline
The AAMC projects a physician shortfall of 86,000 to 124,000 by 2034–2036. The rural impact is disproportionate: approximately 20% of Americans live in rural areas but only ~11% of physicians practice there.
By 2038, HRSA projects nonmetro areas will face a 39% shortage of primary care physicians.
Rural health clinics are federally required to be staffed by an NP, PA, or certified nurse-midwife at least 50% of operating hours. That requirement makes the NP/PA pipeline a direct determinant of whether rural ACOs can sustain care coordination at scale.
Data shows that the rural share of National Health Service Corps clinicians declined from 48% in 2000 to 32% in 2020, even as urban nonphysician primary care density rose.
Payment, Benchmarking, and Data Disadvantages
The benchmarking trap:
Because rural ACOs often represent a large share of their region's Medicare patients, when they successfully reduce spending, they simultaneously lower their own regional benchmarks. The savings achievement becomes a penalty.
Research published in Health Affairs found that for every $100 an ACO's baseline spending was below its region, it remained $92 below in its first 3 performance years — making it progressively harder to meet targets and creating a structural disincentive to improve.

The risk adjustment problem:
Current methodology does not fully capture the social complexity of caring for rural patients — food deserts, travel distances, limited behavioral health access. This makes rural ACO performance appear weaker on paper than it actually is relative to urban peers.
The data lag challenge:
Rural ACOs face compounding data problems at every level:
- Claims data delays: CMS data can arrive months late, limiting real-time care management decisions
- SDOH collection gaps: Social determinants data remains nascent and inconsistent across ACO sites
- Resource scarcity: Even when social needs are identified, few community resources exist to act on them — making data collection feel futile without parallel investment in community capacity
How Federal Policy Is Responding: MSSP and ACO REACH
MSSP Reforms Effective Since 2023
The Calendar Year 2023 Medicare Physician Fee Schedule final rule introduced several reforms to support rural and underserved ACOs:
Advance Investment Payments (AIP):
- One-time upfront payment of $250,000 plus risk-adjusted quarterly per-beneficiary payments for the first two years
- Targets low-revenue/new entrant ACOs serving underserved beneficiaries
Benchmarking adjustments:
- Negative regional adjustment cap reduced from 5% to 1.5% of national per capita Part A and B expenditures
- Further tapering based on dual-eligible share and risk scores
Risk scoring policy:
- 3% aggregate cap across all enrollment types
- Accounts for demographic risk score changes prior to applying the HCC cap
Health equity quality bonus:
- Up to 10 bonus points in the MIPS quality performance category for high-quality reporting and serving underserved beneficiaries
- Uses measures such as Area Deprivation Index (ADI), Low-Income Subsidy (LIS), and dual eligibility

Where MSSP targets financial incentives, ACO REACH goes a step further — embedding equity directly into how benchmarks are set and how care is structured.
ACO REACH's Structured Health Equity Framework
The ACO REACH model builds equity into its core design:
Health Equity Benchmark Adjustment (HEBA):
- Adjusts benchmarks based on a beneficiary-level equity score incorporating ADI (national and state-level) and low-income markers (dual eligibility and Part D LIS)
- Raises the target for ACOs serving the most underserved beneficiaries
Health Equity Plans:
- Identification of underserved populations is mandatory
- Implementation strategies must include measurable goals
- Use of standardized data elements for low-income/ADI factors
Expanded NP scope of practice:
- NPs treated as primary care specialists for alignment
- Beneficiaries can voluntarily align to NPs
- NPs participate in Primary Care Capitation payment mechanics
The Critical Limitation Both Models Share
ACO leaders report that even well-designed financial incentives cannot overcome community resource scarcity. When Meals-on-Wheels has a six-month waitlist and the nearest behavioral health specialist is 60 miles away, a better benchmark doesn't move the needle. What fills that gap is knowing which providers exist, where they're at risk of leaving, and how to recruit into the void — exactly the kind of workforce intelligence that ACO financial design cannot supply on its own.
Closing the Rural Workforce Data Gap
While SDOH data collection and patient-level risk stratification have received growing attention in ACO policy, a foundational and underappreciated barrier to rural ACO performance is incomplete data on the healthcare provider (HCP) workforce itself.
Without knowing the actual supply, distribution, and retention rates of MDs, NPs, and PAs across rural counties, ACOs and state-level programs cannot reliably plan care coordination capacity or anticipate shortfalls before they become crises.
Physician and NP/PA shortages are not static — they shift year over year as providers retire, relocate, or burn out. Rural ACOs without current, measurable workforce baseline data cannot set realistic targets or demonstrate improvement to CMS and state partners.
HealthFront Baseline™: AI-Native Rural HCP Workforce Data Infrastructure
HealthFront Ventures developed HealthFront Baseline™ to address this gap directly. It is an AI-native rural HCP workforce data infrastructure delivering four quantitative metrics plus one Rural County Quality Measure — giving rural healthcare organizations, state-level Rural Health Transformation programs, and ACO administrators the standardized baseline data needed for evidence-based recruitment, retention planning, and care coordination strategy.
The service launches Q1 2026 with FY25 baseline data, providing outsourced data warehouse and lake infrastructure that eliminates the need for custom builds. HealthFront Baseline™ focuses specifically on the measurable rural HCP workforce — MDs and NPs/PAs — enabling rural ACOs to:
- Identify county-level provider supply gaps
- Track workforce retention and attrition patterns
- Set recruitment targets aligned with care coordination goals
- Demonstrate measurable progress to CMS and state partners

This data infrastructure complements the policy reforms in MSSP and ACO REACH by ensuring rural ACOs have the workforce intelligence needed to put equity-focused care coordination into practice.
Frequently Asked Questions
What is an Accountable Care Organization (ACO)?
ACOs are voluntary groups of doctors, hospitals, and providers that coordinate care for Medicare patients, with payment linked to quality performance and cost efficiency under programs like the Medicare Shared Savings Program (MSSP). They share in savings when they improve quality while reducing spending below regional benchmarks.
How do ACOs help reduce health disparities in rural areas?
ACOs can reduce disparities indirectly through better care coordination, chronic disease management, and outreach — but carry no explicit equity mandate. Research links sustained ACO participation of 3+ consecutive years to measurable reductions in disparities, rather than short-term enrollment.
What makes rural ACOs structurally different from urban ACOs?
Rural ACOs face workforce shortages, geographic barriers to care access, limited post-acute networks, benchmarking systems that penalize efficiency gains, and lower community social service infrastructure compared to urban settings. These structural differences require distinct policy supports and performance expectations.
What is the difference between MSSP and ACO REACH for rural providers?
MSSP is the flagship program with 2023 reforms adding Advance Investment Payments and adjusted benchmarks for underserved ACOs. ACO REACH is a more advanced model with mandatory health equity plans, ADI-adjusted benchmarks, and expanded NP scope of practice built directly into its structure.
How long does it take for ACO participation to show improvements in rural health outcomes?
Most evidence points to at least 3 years of consecutive ACO participation before health outcome improvements become measurable at the patient level. Clinical protocol alignment and organizational change take time — rural disparities rarely narrow before that threshold.
Why does rural HCP workforce data matter for ACO performance and health equity?
Workforce supply — how many MDs, NPs, and PAs are actively practicing in a rural county — directly determines whether ACO care coordination goals are achievable. Without baseline data, organizations have no way to identify shortfalls or measure whether recruitment efforts are closing them.