Introduction
A nurse practitioner in rural Montana logs into her system to treat a patient who recently moved from two states away. The woman's complex medical history spans three different hospital networks, a specialty oncology center, and multiple urgent care visits. None of that information appears in the current EHR. The clinician faces a choice: delay treatment to chase down fragmented records, or make clinical decisions with an incomplete picture. This scenario isn't an edge case — it's the daily reality across rural and underserved healthcare settings.
The Single Patient View (SPV) offers a solution: a unified, continuously updated record of a patient's health data accessible across departments, care settings, and providers. For decades, healthcare IT systems have promised integration, yet most organizations still operate on batch processing and legacy messaging that refreshes data periodically — not continuously. The result is stale, siloed datastores where no single system holds the full clinical picture.
The scale of this problem is measurable. According to a study published in PLOS ONE, 58.1% of U.S. inpatient super-utilizers received care at more than one hospital in a single year, with 30-day readmissions climbing to 70.2% among the most fragmented patients.
Data streaming — the continuous, real-time ingestion and processing of patient data — is the infrastructure layer that finally makes SPV achievable. The sections below break down how this technology works in practice and how rural healthcare organizations can adopt it without standing up a dedicated data engineering team.
Key Takeaways
- Healthcare data lives in siloed legacy systems that communicate in batch mode, creating incomplete patient records at the point of care
- Data streaming continuously ingests from EHRs, labs, wearables, and clinical feeds into one unified, real-time patient record
- Interoperability, HIPAA compliance, and scalability challenges each have well-defined solutions within modern streaming architectures
- Real-world applications include clinical trial matching, chronic disease monitoring, and real-time medication safety alerts
- Rural organizations face the steepest SPV barriers and gain the most from unified patient data
- Outsourced AI-native data infrastructure eliminates the need for internal data engineering teams
What Is the Single Patient View — and Why Most Healthcare Systems Fall Short
A Single Patient View is a unified, real-time longitudinal record that integrates every element of a patient's clinical history: diagnoses, medications, allergies, lab results, imaging, specialist visits, and care episodes — across every provider touchpoint, facility, and payer. Unlike an EHR, which captures one organization's view of the patient, SPV aggregates data across all systems, giving clinicians a full, cross-system view of the patient's history regardless of where care was delivered.
Most healthcare IT infrastructures fail to deliver SPV because they were built on batch processing and legacy HL7 v2 messaging. Data updates happen periodically — nightly, hourly, or at best every few minutes — not continuously. The result is a patchwork of disconnected systems where each holds a fragment of the truth, but none holds the whole story.
Those gaps have direct clinical consequences. In a national physician survey, 23.9% reported at least one EMR-related patient safety incident in a 4-week period, with 8.8% of incidents attributed to interoperability and system integration failures — missing data, unsynced records, and incomplete medication histories that contributed to outcomes ranging from treatment delays to death. Duplicate testing, medication errors from incomplete allergy records, and delayed diagnoses are not edge cases; they are predictable outcomes of fragmented data infrastructure.
The problem compounds in multi-facility and multi-specialty environments. A patient generates records at a hospital ED, a specialist clinic, an independent lab, and a retail pharmacy — none of which automatically share data with the others.
The numbers bear this out. Only 62% of hospitals in 2021 performed all four interoperability domains: send, receive, find/query, and integrate outside data. Even where exchange exists, 57% of hospitals cite patient matching difficulty and 72% report vendor-to-vendor challenges. Without a connecting data layer that normalizes, matches, and streams updates in real time, SPV remains an aspiration rather than a reality.
The Data Sources That Must Feed a True SPV
Achieving SPV requires integrating data from diverse source systems, each with different formats, protocols, and update frequencies:
- EHR/EMR systems — Clinical notes, encounter histories, problem lists, care plans
- Laboratory information systems (LIS) — Lab orders, results, reference ranges
- Pharmacy systems — Medication orders, dispensing records, refill histories
- Imaging systems (PACS) — Radiology and pathology reports, imaging metadata
- Wearable and remote monitoring devices — Vital signs, activity data, glucose readings
- Insurance and claims feeds — Coverage details, authorization status, utilization patterns

Healthcare data standards like HL7 FHIR (Fast Healthcare Interoperability Resources) exist specifically to normalize these diverse formats for exchange. FHIR is designated by ONC as the API-focused standard for representing and exchanging health information through modular, resource-based data models.
The adoption reality is more complicated. More than 80% of Health Information Exchange organizations still routinely use HL7 v2 messaging, with 90% receiving HL7 v2 ADT messages and only about 20% routinely using FHIR APIs.
This means any SPV architecture must bridge HL7 v2, C-CDA documents, proprietary vendor formats, and emerging FHIR APIs into a single unified model — a transformation gap that stream processing can close by translating legacy messages into FHIR resources as data moves through the pipeline.
How Data Streaming Enables a Real-Time Single Patient View
Data streaming is the continuous, real-time ingestion and processing of data as it is generated. Unlike batch processing — where data is collected and processed at scheduled intervals (nightly, hourly) — streaming means a clinician's view of the patient updates the moment new data is created: when a lab result is finalized, when a medication is ordered, when a wearable device transmits a vital sign reading.
At the core of healthcare data streaming is a publish-subscribe (pub/sub) architecture. Source systems publish data events — a new lab result, a medication order, a device reading — to a central streaming platform. Downstream applications subscribe to receive only the relevant data: clinical dashboards pull updates for patients currently in the ED, decision support tools monitor medication orders for interaction alerts, patient portals display new test results. This pub/sub pattern decouples producers from consumers, removing single points of failure and enabling systems to scale independently.
Stream processing transforms, enriches, and routes patient data in real time. Technologies like Apache Flink handle this without human intervention or batch delays — specifically:
- Normalizes raw HL7 v2 messages into FHIR format
- Matches incoming records to the correct patient using master patient index (MPI) logic
- Filters and routes data to the right consuming applications
A real-world oncology SPV built with Apache Flink and Confluent Cloud processes encrypted EMR payloads, transforms them in-stream, and makes normalized FHIR data available to clinical trial matching services and analytics platforms in near real time.
A data streaming platform also serves as a durable data backbone. It retains a replayable log of all patient data events, enabling historical analysis, audit trails, and disaster recovery — essential for HIPAA compliance and data governance. Kafka's durable, replayable log supports HIPAA audit controls by maintaining event histories that can be replayed for compliance reviews or used to rebuild downstream systems after failures.
For organizations that lack internal data engineering capacity — common among rural and community health organizations — building a custom streaming pipeline may not be feasible. Outsourced, AI-native data infrastructure offers an alternative path. HealthFront Ventures' AI-Native HCP Workforce Data Warehouses and Lakes provide pre-built infrastructure that eliminates the need for custom pipeline development, so organizations can achieve data integration goals without hiring specialized data engineering teams.
Rural health organizations face a distinct challenge: managing provider workforce data alongside patient clinical records. HealthFront Baseline™ (launching Q1 2026) addresses the workforce side of this equation, offering foundational quantitative metrics and a Rural County Quality Measure that complement clinical SPV efforts without requiring additional data engineering overhead.
Real-World Clinical Applications Powered by the Single Patient View
Clinical Trial and Treatment Matching
A real-time SPV enables research teams and oncology practices to automatically identify eligible patients for clinical trials based on continuously updated biomarker data, diagnoses, and medical history. Without streaming, this matching process is manual, delayed, and prone to missed candidates — researchers run periodic queries against stale databases and rely on clinicians to remember eligible patients during appointments.
An oncology-focused matching service built on a real-time SPV with Apache Flink and Confluent Cloud replaced batch delays with real-time eligibility alerts delivered directly to practices. When a patient's lab results or genetic test updates their record, the streaming platform immediately re-evaluates trial eligibility and notifies the care team, shortening the time from eligibility to enrollment and connecting more patients to therapies they may otherwise miss.
Real-Time Medication Safety and Clinical Decision Support
An SPV fed by streaming data allows clinical decision support systems to generate real-time alerts the moment a new prescription is entered. For example, a drug-drug interaction alert can fire based on the patient's full, continuously current medication history — including prescriptions filled at external pharmacies and medications prescribed by other providers in different systems.
That real-time accuracy requires the medication record to be continuously current — not refreshed in nightly batches. A streaming SPV ensures that when a rural ED physician prescribes a new antibiotic, the system has access to the patient's recent prescription from a specialist two counties away, flagging potential interactions before the medication is dispensed.
Chronic Disease Management and Remote Patient Monitoring
Wearable devices and remote monitoring tools continuously generate vital sign and activity data. When streamed into an SPV, this data allows care teams to detect deterioration and intervene early.
A 2025 JMIR review documented 37 state Medicaid programs reimbursing remote patient monitoring (RPM), with examples including maternal hypertension programs for predominantly Black, rural, Medicaid-covered populations that reported improvements in medication adherence and shifts from ED visits to elective outpatient care.
Rural patients with chronic conditions often have limited access to in-person follow-up. Continuous data streaming from blood pressure cuffs, pulse oximeters, and glucose monitors — integrated directly into their SPV — enables proactive care management without requiring a clinic visit. Clinicians receive alerts when vital signs cross thresholds, allowing virtual check-ins and medication adjustments before an acute episode requires emergency transport.
Infectious Disease Surveillance and Public Health Response
Real-time streaming from EHRs across facilities enables aggregate population-level insights. A near real-time, EHR-based COVID-19 surveillance system processing approximately 300,000 transactions per day integrated hospital, lab, and primary care data, tracking:
- 72,872 confirmed hospitalized cases
- 12,465 ICU admissions
- 9,019 deaths (as of February 2022)
The system supported bed management, isolation center coordination, automated notifications, and predictive models — all powered by continuous data streaming that detected unusual symptom clusters across regions before formal outbreak declarations.
Navigating the Challenges: Interoperability, Compliance, and Scalability
Interoperability and Data Transformation
Achieving SPV requires more than connecting systems — it requires normalizing their outputs. Many legacy systems produce HL7 v2 messages that must be transformed into FHIR before feeding a unified patient record. Stream processing layers can perform this transformation in-flight, without requiring source system changes.
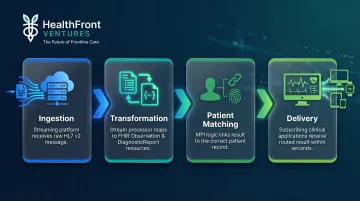
Consider how an HL7 v2 ORU lab result travels through a streaming pipeline:
- A streaming platform ingests the raw HL7 v2 message from the lab system
- A stream processing engine parses and maps it to FHIR Observation and DiagnosticReport resources
- MPI logic matches the result to the correct patient record
- Subscribing clinical applications receive the routed result — within seconds of the lab publishing it
This in-stream transformation bridges the gap between the 80%+ of HIEs still running HL7 v2 and the growing ecosystem of FHIR-native analytics and clinical applications.
HIPAA Compliance and Data Security
A streaming architecture for healthcare must implement strict security controls:
- End-to-end encryption of PHI: The HIPAA Security Rule requires encryption of ePHI in transit and at rest (addressable standard). TLS encryption protects data in motion; encryption at rest protects stored event logs.
- Role-based access controls: Technical access controls are required to ensure only authorized clinicians access specific patient data streams.
- Audit logs: Mechanisms to record and examine activity in systems containing ePHI are required. Streaming platforms' durable logs inherently support this requirement.
HIPAA-compliant certifications such as HITRUST CSF are available for managed streaming platforms and should be a procurement requirement. Organizations evaluating streaming vendors should verify HITRUST certification and review security architecture documentation for compliance with HIPAA technical safeguards.
Scalability and Operational Resilience
Healthcare data volumes are high and throughput is unpredictable. Surges occur during flu seasons, large-scale screening events, or public health emergencies. A streaming architecture must scale elastically to handle peaks without pipeline failures.
Mature streaming platforms address this through several operational capabilities:
- Elastic provisioning: Automatically adds capacity as event volumes spike, then scales down during normal periods to control costs
- Cross-region replication: Mirrors cluster data across geographies so infrastructure failures in one region don't interrupt patient data access
- Durable event logs: Retain messages through processing delays or downstream outages, preventing data loss during recovery
For SPV to function at the point of care, clinicians need confidence that patient data arrives reliably — whether the system is handling routine Monday morning census loads or a regional mass-casualty surge. Operational resilience is what makes that confidence possible.
Special Considerations for Rural Healthcare Organizations
Rural healthcare organizations face a compounded version of the SPV challenge. Fewer providers serve larger geographic areas. Patients often travel across county or state lines for specialty care, generating records at facilities with no direct data exchange relationships. Rural areas have 5.1 primary care physicians per 10,000 population compared to 8.0 in urban areas, increasing the likelihood that a patient's care is split across multiple unconnected systems.
The infrastructure gaps compound the data challenge:
- EHR adoption rates are lower in rural settings, with many facilities still relying on paper records or legacy systems
- Limited interoperability capabilities restrict data exchange even when digital records exist
- IT staff are scarce — rural hospitals and clinics rarely have dedicated data engineering teams
- Few organizations have the internal capacity to build and maintain custom streaming pipelines

State-level Rural Health Transformation (RHT) programs prioritize data interoperability and unified patient records as prerequisites for improving care quality and provider retention. HRSA's National Advisory Committee on Rural Health and Human Services highlighted opportunities to connect rural providers with digital innovations and recommended actions to strengthen rural tech capacity.
CMS's Interoperability and Prior Authorization Final Rule advances API-enabled data exchange to reduce administrative burden and improve timely access to patient information — signaling continued federal investment in rural data infrastructure.
These federal tailwinds create real opportunity — but most rural organizations still lack the internal resources to act on them. Outsourced data infrastructure with pre-built connectors and baseline metrics removes the barrier of needing an in-house data engineering team.
HealthFront Baseline™ (launching Q1 2026) provides foundational quantitative metrics and a Rural County Quality Measure that can anchor clinical SPV efforts. Rural organizations can use that same infrastructure to measure provider workforce distribution and patient access patterns — without standing up a custom data platform.
Frequently Asked Questions
What is streaming data integration?
Streaming data integration is the continuous, real-time process of connecting and synchronizing data from multiple source systems as data is generated, rather than at scheduled intervals. For healthcare SPV, this ensures patient records are always current, updating the moment new clinical data is created.
How does HIE differ from EHR?
An EHR (Electronic Health Record) is a system used by a single organization to record patient care. An HIE (Health Information Exchange) is a network enabling multiple organizations to securely share patient data across systems. Data streaming can connect both into a unified SPV.
What is a Single Patient View in healthcare?
A Single Patient View is a unified, real-time longitudinal record consolidating a patient's clinical data from all care touchpoints: hospitals, clinics, labs, pharmacies, and specialists. That complete picture is what enables accurate clinical decisions, coordinated care, and fewer preventable errors.
What role does FHIR play in healthcare data streaming?
FHIR (Fast Healthcare Interoperability Resources) is the modern standard for structuring and exchanging healthcare data. Streaming platforms use FHIR as the normalized output format so diverse source systems can feed a unified patient record without requiring point-to-point integrations.
How does data streaming improve patient outcomes in rural healthcare?
Rural patients often receive care across multiple sparse facilities. Data streaming ensures that regardless of where a patient was last seen, their treating provider has a current, complete record, which cuts duplicate testing, reduces missed diagnoses, and helps prevent medication errors.
What are the biggest barriers to implementing data streaming for a Single Patient View?
The main barriers include legacy system interoperability, HIPAA compliance complexity, limited internal data engineering capacity, and custom infrastructure costs. Managed data infrastructure services lower these barriers for smaller organizations by eliminating the need for custom builds from scratch.