Introduction
Rural healthcare organizations face an existential challenge: 92% of rural counties are designated primary care Health Professional Shortage Areas, and 199 rural counties have no primary care physicians at all. As patient populations age, demand for services climbs, and the clinical workforce shrinks, workforce planning has shifted from a discretionary HR function to a survival imperative.
The distinction between reactive staffing—filling gaps as vacancies appear—and proactive strategic workforce planning matters more in rural settings than anywhere else. A single unfilled MD, NP, or PA vacancy can disrupt care access for an entire county, driving patients to distant emergency rooms or forcing them to delay treatment altogether.
Rural healthcare organizations that get ahead of these shortages share one common trait: they plan before the crisis arrives, not after.
TLDR:
- The U.S. faces a projected shortage of up to 86,000 physicians by 2036, with rural areas hit hardest
- Strategic workforce planning analyzes capacity, forecasts needs, and builds retention and recruitment strategies
- Effective plans rely on baseline metrics, scenario modeling, and AI-powered demand forecasting
- Outsourced data infrastructure helps rural organizations skip costly custom builds
- Continuous monitoring and iteration determine whether a workforce plan delivers results or stalls
What Is Healthcare Workforce Planning?
Healthcare workforce planning is the process of analyzing current workforce capacity, forecasting future staffing needs, identifying gaps, and developing strategies to ensure the right number of qualified clinical and support staff are available at the right time and place. It transforms workforce management from a reactive scramble into a strategic capability aligned with organizational goals.
Workforce Planning vs. Workforce Management
These terms are often confused, but they serve distinct purposes:
- Workforce planning: Strategic, long-range, tied to clinical service goals and community health needs. Answers questions like "How many primary care providers will we need in three years?" and "What retention incentives will reduce NP turnover?"
- Workforce management: Operational, day-to-day scheduling and deployment. Focuses on shift coverage, PTO requests, and float pool assignments.
The two are related but occupy different time horizons. Planning sets the strategic direction; management executes daily operations within that framework.
Integrated Workforce Planning
Integrated workforce planning aligns workforce strategy with clinical service goals, financial planning, community health needs, and population demographics. Instead of isolated HR-driven headcount projections, integrated planning connects workforce decisions to tangible outcomes:
- Expanding a diabetes management program requires endocrinologists or NPs with chronic disease expertise — not general headcount
- Recruitment budgets must align with reimbursement projections and operating margins, not run parallel to them
- An aging service area population demands geriatric capacity; population trends should drive specialty mix
- Local workforce supply, HPSA designations, and rural-urban migration patterns define what's actually achievable
Without that integration, staffing models drift from clinical reality — organizations hire for yesterday's service mix while tomorrow's patient population goes underserved.
Why Strategic Workforce Planning Is Critical Right Now
The U.S. healthcare system faces a projected shortage of between 13,500 and 86,000 physicians by 2036, with primary care accounting for 20,200 to 40,400 of that shortfall. These aren't abstract projections—they translate directly into operational risk for organizations without a plan.
Compounding Workforce Pressures
Historical staffing baselines no longer provide reliable guidance. Multiple forces converge to make forward-looking, data-informed approaches essential:
- Workforce aging: 42% of active physicians are nearing retirement, with 23.4% already age 65 or older
- Burnout and attrition: More than one-third of burned-out primary care physicians plan to stop seeing patients, amplifying projected shortages beyond demographic retirement trends
- Rising patient acuity: Sicker, more complex patients require more clinician time per visit
- Post-pandemic demand patterns: Deferred care during COVID created backlogs that persist well into the current decade, with no clear resolution timeline in high-need areas
Organizations relying on 2019 staffing models to plan for 2026 needs are planning with obsolete data.
Disproportionate Rural Impact
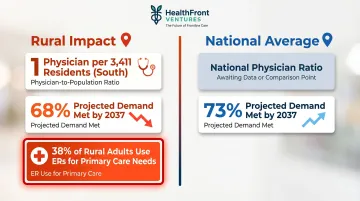
Those obsolete models hit rural communities hardest. In the South, the average ratio is 1 primary care physician per 3,411 rural residents — a baseline that's already strained. HRSA projects rural areas will meet only 68% of primary care physician demand by 2037, compared to 73% nationally.
The consequences are measurable: 38% of rural adults use emergency rooms for care that a primary care provider could handle. That pattern drives higher costs, worse outcomes, and measurable deterioration in community health — all directly traceable to workforce gaps. For rural healthcare providers, getting workforce planning right is less about competitive advantage and more about organizational survival.
The Biggest Challenges in Healthcare Workforce Planning
Structural Supply-Demand Imbalances
The healthcare talent pipeline cannot scale fast enough to match demand. U.S. medical school enrollment reached 99,562 students in 2024-25—approximately 40% growth since 2002—but the Medicare-funded GME residency cap remains the binding constraint on physician supply growth. Congress authorized just 200 new Medicare GME positions in November 2024, a fraction of what's needed.
Even when clinicians exist nationally, geographic concentration in metro areas leaves rural communities underserved. The proportion of National Health Service Corps clinicians practicing in rural areas dropped from 48% in 2000 to 32% in 2020, even as the total NHSC count grew from 900 to 15,637. This reveals a critical reality: aggregate supply growth doesn't translate to rural supply growth without explicit geographic targeting.
Nurse practitioners and physician assistants represent a promising expansion path. BLS projects NP employment to grow 40% from 2024 to 2034, adding 128,400 new positions. Yet geographic distribution affects advanced practice providers too: only 14.38% of surveyed NPs practice in rural areas versus 85.62% in urban areas.
Retention and Burnout Pressures
Turnover is as much a planning challenge as recruitment. National hospital RN turnover was 16.4% in 2024, down from pandemic peaks but still elevated above historical norms. Unplanned vacancies cascade into understaffing, heavier loads for remaining staff, and further turnover—a self-reinforcing cycle.
Burnout drives much of this attrition. Primary care physicians in the VHA hit 57.6% burnout in 2022, the highest of any occupational group. Organizations that focus exclusively on recruitment while ignoring retention incentives, scheduling flexibility, and career development tend to fail—especially in rural settings where competitive compensation is harder to match.
Rural NPs already work longer hours (40.19 vs. 36.41 hours/week for urban NPs) and manage patient panels more autonomously. Absorbing additional workload when vacancies occur accelerates burnout in the providers you can least afford to lose.
Data and Infrastructure Gaps
Many organizations lack standardized ways to measure current workforce composition, turnover risk, or demand projections—especially at the county or regional level. Without reliable baseline data, leadership cannot build credible forecasts or measure progress against goals.
Data silos make this worse. HR systems, EHRs, credentialing databases, and financial systems rarely integrate, which means decision-makers are working from incomplete pictures:
- A CFO sees labor cost per patient visit — but not whether high costs stem from overstaffing, overtime, or travel clinician reliance
- An HR director tracks vacancy rates — but not how those vacancies correlate with patient volume surges or seasonal demand
- A clinical leader monitors scheduling gaps — but not the downstream financial impact on the organization
When workforce data can't connect to operational and financial outcomes, planning decisions default to gut instinct rather than evidence. That's a costly gap to leave unfilled.
Key Elements of an Effective Healthcare Workforce Plan
Workforce Demand Assessment
Understanding demand means more than headcount. It requires analyzing:
- Patient volume trends: Are visits growing, stable, or declining by service line?
- Acuity levels: Sicker patients require more clinician time per encounter
- Seasonal fluctuations: Flu season, summer tourism, agricultural cycles
- Community demographics: Population growth, aging trends, chronic disease prevalence
- Service line expansion: New services require new skills and credentials
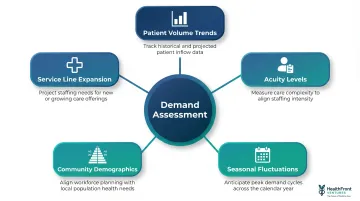
A rural health system planning to expand behavioral health services needs psychiatric NPs or licensed clinical social workers, not additional family medicine providers. Demand assessment connects staffing to the actual services the community needs.
Once demand is understood, the next step is an honest look at what you actually have — and what the external market can realistically provide.
Workforce Supply Analysis
The supply-side assessment inventories current resources and evaluates external talent markets:
- Current staff by role and credential: How many MDs, NPs, PAs, RNs by specialty and department?
- Retirement risk: What percentage of your workforce is within five years of retirement age?
- Turnover probability: Which departments show elevated attrition in exit interviews?
- Skills gaps: Do you have capacity in high-acuity specialties (critical care, oncology, cardiology)?
- External talent market: What's the regional and national supply of candidates for hard-to-fill roles?
For rural organizations, external talent market analysis must account for geographic clustering. National supply figures are irrelevant if most candidates won't relocate to rural areas.
Baseline Metrics and Performance Benchmarks
Without knowing where you are today, you cannot measure progress or make credible projections. Foundational metrics include:
- Vacancy rates by role: What percentage of budgeted positions are unfilled?
- Time-to-fill: Median time to fill a primary care physician position is approximately 93 days nationally, but rural practices face materially longer timelines
- Turnover rate by department: Where is attrition highest?
- Nurse-to-patient ratios: Are you meeting safe staffing benchmarks?
For rural healthcare organizations that need structured baseline data without building custom analytics infrastructure, HealthFront Baseline™ provides a ready-to-use starting point. The service delivers four quantitative workforce metrics plus a rural county quality measure, calibrated for rural HCP (MD, NP, PA) workforce planning at the state and county level.
Scheduled to launch in Q1 2026 with FY25 baseline data, HealthFront Baseline™ eliminates the need to build proprietary measurement systems from scratch.
Gap Analysis and Scenario Planning
Once you understand demand and supply, identify specific workforce gaps—both current shortfalls and projected future gaps. Use scenario modeling to stress-test assumptions:
- What happens if two key NPs resign within 12 months?
- How does patient volume growth of 15% over three years affect staffing needs?
- What if Medicare reimbursement rates change and force budget cuts?
Each scenario should produce a specific contingency: a hiring trigger, a contract staffing threshold, or a service-line adjustment — not just an awareness that a risk exists.
Action Planning for Retention and Recruitment
Structured retention and recruitment plans translate gap analysis into concrete interventions:
- Are salaries competitive with regional and national markets? Compensation benchmarking answers this directly.
- NHSC and state-funded loan repayment programs remain among the highest-ROI rural recruitment tools available.
- Internal NP/PA training pipelines reduce long-term dependence on external hiring.
- Partnerships with local universities and residency programs build a candidate pipeline before vacancies open.
- Scheduling flexibility and structured career development paths rank consistently in rural provider retention surveys.
HealthFront Ventures offers Retention & Recruiting Incentive Structured Planning as a dedicated service, focused specifically on expanding the rural NP/PA workforce through data-driven incentive strategies. The output is a prioritized action plan tied to your county-level workforce data — not a generic retention checklist.
The Strategic Workforce Planning Process: A Step-by-Step Approach
Step 1: Define Scope, Ownership, and Goals
The planning process begins with clarity:
- Who owns the plan? HR, clinical leadership, or a joint task force?
- What scope does it cover? Single facility, regional network, or state-level initiative?
- What strategic goals does it support? Aligning workforce planning to organizational mission from the start ensures the plan drives real outcomes rather than sitting on a shelf
Without clear ownership, workforce plans become orphaned documents no one implements.
Step 2: Collect and Analyze Workforce Data
Gather internal and external data to build a coherent picture of current state:
Internal data:
- Current FTEs by role and department
- Turnover history and exit interview findings
- Retirement projections
- Credentialing and licensure status
External data:
- Regional labor market supply
- HPSA designations and rural health rankings
- Educational pipeline output (local nursing and PA programs)
- Competitor staffing levels and compensation
Pull these inputs together into a baseline assessment that quantifies where you stand today.
Step 3: Identify Gaps and Prioritize Risks
Translate data analysis into a prioritized gap assessment. Which roles, departments, or geographies carry the most risk?
Focus on:
- Roles with highest vacancy rates and longest time-to-fill
- Departments with elevated turnover and burnout indicators
- Service lines critical to financial sustainability or community health outcomes
Set planning priorities rather than trying to solve every problem at once. A rural health system with a 30% NP vacancy rate and stable RN staffing should prioritize NP recruitment over RN pipeline development.
Step 4: Develop and Implement Targeted Interventions
Each gap identified in Step 3 should map to a specific intervention. Common options include:
- Proactive recruitment pipelines: Ongoing candidate relationship-building, not just posting openings when vacancies occur
- Retention incentive structures: Compensation, benefits, and non-financial incentives (autonomy, flexible scheduling, mission-driven work)
- Upskilling and internal mobility: Cross-training RNs to transition into NP roles through employer-sponsored education
- Flexible staffing models: Float pools, per diem staff, and short-term travel clinicians to cover gaps while permanent hires are recruited
- Community and academic partnerships: Hosting clinical rotations and residencies builds future recruitment pipelines
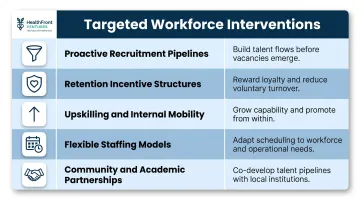
Each intervention should have clear accountability for execution.
Step 5: Monitor, Measure, and Iterate
Plans that don't get measured don't get improved. Establish KPI dashboards to track:
- Time-to-fill by role
- Turnover rate by department
- Labor cost per patient visit
- Vacancy rate (percentage of budgeted positions unfilled)
Set review cadences quarterly at minimum, using real-time data to adjust strategy as conditions shift.
When a metric moves—say, time-to-fill for primary care physicians climbing from 90 to 120 days—investigate root causes immediately rather than waiting for the next annual planning cycle.
The Role of Data and Technology in Modern Healthcare Workforce Planning
AI-powered demand forecasting and predictive analytics have shifted workforce planning from reactive reporting to genuine anticipation. Modern systems project what will happen next quarter by processing:
- Historical patient volumes and seasonal patterns
- Local demographic trends and population growth
- Staff utilization rates and productivity benchmarks
- Regional labor market supply and competitor hiring activity
That capability gap is significant. Approximately 80% of healthcare organizations identify AI as a top strategic priority, yet only 30% of large health systems actually use AI for workforce management. For rural providers, the gap between aspiration and execution is wider still.
Barriers for Rural Organizations
Rural hospitals face steeper adoption barriers than urban counterparts:
- Budget constraints: 72% of rural hospitals cite budget limitations as AI adoption barriers
- Lack of technical staff: 60% lack the internal capacity to implement and maintain AI-driven tools
- Data infrastructure gaps: For every $1 spent on an AI tool, organizations often spend $2 to $3 on data cleaning, integration, and training
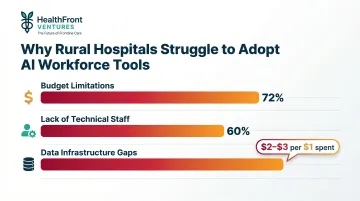
Urban academic centers are three times more likely to have formal AI governance structures. This creates a clear gap: the organizations with the greatest workforce planning needs have the least capacity to implement modern planning tools.
Outsourced Data Infrastructure
Outsourced data infrastructure reduces the time and cost to establish credible, data-driven workforce planning foundations. HealthFront Ventures' AI-native HCP Workforce Data Warehouses and Lakes are built specifically for rural MD and NP/PA workforce planning, eliminating the need for custom data builds and delivering structured workforce intelligence calibrated for rural contexts.

These solutions handle the complete data lifecycle — from acquisition and normalization through analytics-ready datasets — without requiring rural organizations to build proprietary infrastructure. For state-level rural health transformation programs, this means deploying workforce planning capabilities in months rather than building them internally over years at substantial cost.
Technology Considerations for Healthcare Leaders
When evaluating workforce planning tools, prioritize:
- Integration: Confirm it connects natively with your EHR, HRIS, and credentialing platforms — not just through manual exports.
- Compliance: Verify it meets HIPAA, credentialing data handling, and applicable state privacy requirements before any data is shared.
- Transparency: Can you understand how AI-generated recommendations are produced?
- Geographic configuration: Confirm you can configure metrics at the county or regional level — generic statewide averages won't support rural-specific decisions.
Technology that works for a 500-bed urban academic medical center won't suit a 25-bed critical access hospital serving three rural counties. Rural-specific planning requires rural-calibrated tools.
Frequently Asked Questions
What is healthcare workforce planning?
Healthcare workforce planning is the strategic process of analyzing current and future staffing needs, identifying supply-demand gaps, and developing action plans to ensure the right clinical and support staff are available to deliver quality care when and where patients need it.
What is the strategic workforce planning process in healthcare?
The process moves through five stages: defining scope and goals, collecting workforce data, identifying gaps, developing retention and recruitment interventions, and monitoring outcomes. Unlike a one-time plan, it requires regular updates as conditions shift.
What are the key elements of healthcare workforce planning?
The five essential elements are: demand assessment, supply analysis, baseline metrics and benchmarking, gap identification and scenario planning, and targeted recruitment and retention action plans. Each element builds on the last to create a complete picture of your workforce position.
What is integrated workforce planning?
Integrated workforce planning aligns workforce strategy with clinical, financial, and community health goals—breaking down silos between HR, operations, and clinical leadership to create a unified, organization-wide approach rather than isolated headcount projections.
Why is healthcare workforce planning especially challenging in rural areas?
Rural planning faces compounding challenges: geographic maldistribution of clinicians (most cluster in metro areas), limited ability to match urban compensation, smaller local talent pipelines, and the outsized impact of a single vacancy on community care access. A single unfilled primary care role can disrupt an entire county's healthcare delivery.
What data is needed for effective healthcare workforce planning?
Core data categories include FTE counts by role, vacancy and turnover rates, retirement risk projections, regional labor supply, patient volume trends, and county-level quality benchmarks. Organizations without this baseline cannot build credible forecasts or identify where interventions will have the most impact.