Introduction
When rural healthcare organizations enter value-based care contracts, SDOH data gaps can undermine risk stratification, quality scores, and cost targets before a single patient encounter takes place. Yet not all analytics platforms are built to address these gaps equally — especially in rural settings where social risk burden is highest and data infrastructure is thinnest.
The stakes are real: choosing the wrong SDOH analytics solution can mean incomplete population profiles, failed quality metrics, and missed reimbursement. A 2022 HHS evidence review found that clinical care explains only about 20% of county-level variation in health outcomes, while SDOH account for as much as 50%.
When half of your outcomes hinge on non-clinical factors — housing, food access, transportation, economic stability — your analytics platform must capture and operationalize that reality, not just screen for it.
That gap between screening and action is where most platforms fall short. This guide gives rural health organizations, ACOs, and state RHT programs a structured evaluation framework for selecting an SDOH analytics vendor — or deciding whether to build internally. Each question ties analytics capabilities to VBC outcomes, operational feasibility, and health equity goals you can actually measure.
Key Takeaways
- SDOH analytics turns social risk data into clinical and financial decisions that directly shape value-based contract performance
- Strong evaluation frameworks test six critical capabilities: data standardization, EHR integration, rural population support, VBC tracking, closed-loop referrals, and governance
- For rural organizations, sparse data infrastructure and underrepresentation in standard SDOH datasets create compounding evaluation risks
- The right platform prevents costly implementation failures and performance gaps under value-based contracts
- Use this guide as a structured procurement checklist when assessing SDOH analytics vendors
What Is SDOH Analytics in Value-Based Care?
SDOH analytics is the systematic collection, integration, and analysis of non-medical social data across the five Healthy People 2030 domains — economic stability, education access and quality, healthcare access and quality, neighborhood and built environment, and social and community context. It does three things: predicts health outcomes, targets interventions, and supports the value-based performance benchmarks that increasingly require SDOH documentation.
That's where value-based care analytics enters the picture. These models tie reimbursement directly to care quality, patient outcomes, and cost efficiency — and SDOH data has become a required input for accurate risk adjustment and equitable quality measurement under CMS frameworks.
Without it, organizations face penalties, skewed risk scores, and missed shared savings.
Why SDOH Analytics Matters in Value-Based Contracts
Value-based care models — ACOs, MSSP, ACO REACH, and other CMMI programs — are increasingly requiring SDOH screening and documentation. Organizations that fail to capture and act on this data face:
- Quality score penalties
- Risk adjustment inaccuracies
- Missed shared savings
- Lower Star ratings in Medicare Advantage plans
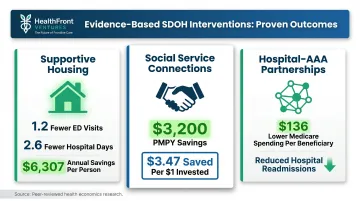
When SDOH data is captured and operationalized, it enables earlier interventions that reduce avoidable utilization. Evidence from the 2022 ASPE review demonstrates measurable impact:
- Supportive housing programs: 1.2 fewer ED visits and 2.6 fewer hospital days per person-year, with average savings of $6,307 annually
- Social service connections: $3,200 per member per year savings; $3.47 in savings per $1 invested
- Hospital-AAA partnerships: $136 lower Medicare spending per beneficiary and reduced readmissions
These programs also improve HEDIS measures. The HEDIS Social Need Screening and Intervention (SNS-E) measure tracks screening for food insecurity, housing needs, and transportation, plus whether interventions occurred within 30 days after a positive screen — creating direct accountability for closing social risk gaps.
Key Questions to Ask When Evaluating SDOH Analytics for Value-Based Care
The following questions form a practical procurement and program evaluation checklist. They help organizations move beyond feature comparisons to connect analytics capabilities to measurable VBC outcomes, health equity goals, and operational feasibility.
Does the platform capture and standardize data across all five SDOH domains?
Why domain completeness matters: Partial SDOH data creates blind spots in risk stratification and produces inequitable care plans. A platform that only screens for food insecurity and transportation misses housing instability, economic strain, and safety risks that drive utilization just as strongly.
Questions to ask vendors:
- Does the platform support ICD-10-CM Z-code documentation (Z55–Z65)?
- Which validated screening tools are supported — PRAPARE, AHC HRSN, AAFP EveryONE?
- How is data from multiple sources (patient surveys, community data, claims) reconciled into a unified patient record?
Performance metrics affected: This influences social risk score accuracy, Z-code capture rates, and HEDIS SNS-E measure compliance. Note that Z-code documentation rates remain extremely low: only 1.59% of Medicare FFS beneficiaries had a Z-code claim in 2019, and 0.94% of MA enrollees in 2017 — indicating that screening alone without structured documentation fails to generate quality measurement or risk adjustment outcomes.
How does the platform integrate with existing EHR and clinical workflows?
SDOH analytics only drives action when embedded into the clinical encounter, not siloed in a separate dashboard. Research published in the Journal of Medical Internet Research found that EHR-integrated SDOH tools increased screening rates from 0.4% to 15.9% in ambulatory settings and from 0% to 66% in inpatient settings. Across six studies, the pooled mean increase in screening rates was 47%.
Questions to ask vendors:
- What EHR interoperability does the platform offer (Epic, Cerner, etc.)?
- Can SDOH screening be triggered within existing workflows, or does it require staff to leave the EHR?
- How do identified needs surface in care manager work-lists and treatment plans?
Performance metrics affected: SDOH screening completion rates, time-to-intervention after screening, and provider adoption rates. Without workflow integration, Z-code documentation rates remain negligible, and SDOH data becomes a compliance exercise rather than a clinical tool.
How does the platform address rural and geographically dispersed populations?
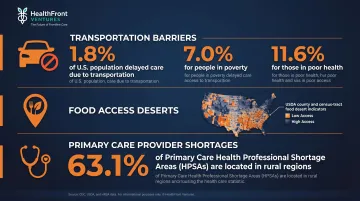
Rural populations carry disproportionate social risk burdens — transportation barriers, food deserts, provider shortages — yet are chronically underrepresented in standard SDOH data sets.
Evidence of rural SDOH burden:
- Transportation: 1.8% of the US population delayed medical care due to lack of transportation in 2017, with much higher rates among people in poverty (7.0%) and those in poor health (11.6%)
- Food access: The USDA Food Access Research Atlas provides county- and census-tract-level indicators for low access and rural food deserts
- Provider shortages: 63.1% of designated primary care HPSAs are in rural areas, according to HRSA
Questions to ask vendors:
- Does the platform offer county- or census-tract-level social risk mapping?
- Does it account for rural-specific data sparsity and limited HCP workforce that directly affect care access as an SDOH variable?
- Can the platform integrate rural-specific data layers, such as provider availability metrics?
HealthFront Baseline™ provides AI-native rural HCP workforce data (MDs, NPs/PAs) with quantitative metrics and a Rural County Quality Measure. For organizations that need to account for provider availability as a structural social determinant, it fills a gap that most SDOH platforms leave unmeasured.
What analytics capabilities support value-based performance tracking?
A VBC-ready SDOH platform must deliver risk stratification outputs, cohort segmentation by social risk profile, and trend tracking against quality benchmarks — not just raw screening data.
Questions to ask vendors:
- What specific VBC performance indicators does the platform support (Star ratings, HEDIS measures, shared savings calculations)?
- How do SDOH risk scores interact with clinical risk scores?
- Does the platform produce audit-ready reporting for CMS or payer submissions?
Performance metrics affected: Star ratings, quality bonus payments, shared savings calculations, and ACO REACH or MSSP benchmark performance. A 2026 JAMA Health Forum analysis found that 46% of MA contracts became bonus-eligible in at least one year specifically due to the Categorical Adjustment Index for social risk. Accurate SDOH capture carries direct financial consequences.

Does the platform support closed-loop referral tracking and community resource linkage?
Identifying SDOH needs without connecting patients to resources and confirming follow-through is a documented failure point. The CMS Accountable Health Communities evaluation screened nearly 483,000 beneficiaries — 15% were eligible for navigation.
Yet only 14% of referred beneficiaries had needs resolved, and 33% were lost to follow-up entirely.
Questions to ask vendors:
- Does the platform include a community resource directory?
- Does it track referral status from initiation to confirmed access?
- Does it support bidirectional data exchange with community-based organizations or social prescribing networks?
Performance metrics affected: Referral uptake rates, unmet social need resolution rates, and downstream reduction in avoidable utilization. Organizations without closed-loop tracking cannot demonstrate SDOH program ROI to value-based payers.
What are the platform's data governance, privacy, and scalability standards?
SDOH data is sensitive and subject to HIPAA. When collected as part of treatment, payment, or operations, it is protected health information. Yet ethical risks exist: stigmatization, retraumatization, and misuse of social risk data in clinical documentation.
Questions to ask vendors:
- What is the data security architecture?
- How does the platform manage consent and patient control over SDOH data?
- How does the vendor handle ethical risks of stigmatization or misuse?
- Can the platform grow from a single clinic to a multi-site state-level program without requiring a complete rebuild?
Performance metrics affected: Audit compliance, patient trust and screening response rates, and total cost of ownership over time. Organizations building toward state-level Rural Health Transformation programs need infrastructure that scales without custom builds for each deployment.
How HealthFront Ventures Can Help
HealthFront Ventures is built specifically for rural healthcare organizations navigating value-based transformation. Its AI-native HCP workforce data infrastructure addresses a gap that most SDOH analytics platforms miss entirely: the availability of the rural provider workforce itself.
HealthFront Baseline™ delivers FY25 Baseline Data Metrics (launching Q1 2026) with four quantitative workforce metrics and one Rural County Quality Measure. Rural health programs and state RHT initiatives get a standardized, outsourced data foundation to benchmark provider retention, recruitment, and availability — no custom infrastructure required.
Key differentiators:
- AI-native HCP workforce data warehouses and lakes designed for rural MDs and NPs/PAs
- Outsourced data infrastructure that scales for state-level RHT execution — no custom builds needed
- Structured to support retention and recruiting incentive planning alongside SDOH program design
- Fills the rural workforce capacity gap that most SDOH analytics platforms leave unaddressed

Conclusion
The goal in evaluating SDOH analytics is not to find the most feature-rich platform, but the one aligned with your organization's value-based care contracts, population profile, and operational capacity. For rural organizations, data gaps are structural. Transportation barriers, food deserts, and provider shortages are not edge cases — they define the operating environment.
SDOH analytics evaluation is not a one-time procurement decision. The questions in this guide should be revisited as CMS requirements evolve, as state RHT programs mature, and as the rural HCP workforce landscape shifts. Continuous benchmarking is how rural programs move from documenting disparities to closing them — and from meeting contract thresholds to building the data infrastructure that justifies future investment.
Frequently Asked Questions
What questions to ask about social determinants of health?
Effective SDOH questions span five domains — housing, food security, transportation, utilities, and safety — and should be drawn from validated tools like PRAPARE or the AHC HRSN Screener. The framing of questions matters as much as the content, particularly in building patient trust and avoiding stigmatization.
What is value-based care analytics?
Value-based care analytics is the use of clinical, financial, and increasingly social data to measure whether care delivery is improving outcomes while reducing costs. SDOH data has become a required input for accurate risk adjustment and equitable quality scoring under CMS-linked payment models.
How does using SDOH data enhance the quality of patient care?
SDOH data helps care teams identify non-clinical barriers (food insecurity, lack of transportation, housing instability) that prevent patients from following care plans. Addressing these gaps directly improves treatment adherence, reduces misdiagnosis risk, and strengthens the patient-provider relationship over time.
How does data impact value-based care?
Data is the operational foundation of value-based care: it enables risk stratification, performance benchmarking, quality reporting, and intervention targeting. Without accurate SDOH and workforce data, organizations cannot identify where social risk is driving cost or where care gaps exist.
What are the 5 key needs that contribute to healthcare cost minimizing strategies?
The five SDOH-related needs most linked to healthcare cost are housing stability, food security, transportation access, utility support, and interpersonal safety. Data-driven referral programs targeting these areas reduce ED utilization, readmissions, and chronic disease escalation in value-based models.