Introduction
Only 48% of rural hospitals participated in all four interoperability domains in 2021, compared to 62% nationwide — a gap that creates real safety risks when patient records are incomplete at the point of care.
Behind that gap is a data problem. Most rural healthcare organizations collect substantial information but struggle to translate it into decisions that improve staffing, patient care, and financial sustainability.
A data warehouse isn't just an enterprise IT concept for large health systems. For rural organizations operating with tight margins and limited staff, it's a practical tool for getting accurate records faster, planning workforce needs more precisely, and making better use of constrained resources. This article covers the concrete benefits, real use cases, and what organizations risk by operating without one.
Key Takeaways
- A healthcare data warehouse aggregates data from EHRs, lab systems, claims, and workforce records into one structured platform for analysis
- Faster clinical decisions, population health management, workforce intelligence, and regulatory compliance all improve when data is centralized and structured
- Key use cases include chronic disease management, cost optimization, and provider retention planning — with outsized impact in rural and underserved markets
- Organizations without structured data infrastructure face fragmented reporting, reactive decision-making, and rising operational costs
- Outsourced, AI-native solutions like HealthFront Baseline™ deliver full-scale data capabilities without requiring custom infrastructure builds
What Is a Healthcare Data Warehouse?
A healthcare data warehouse is a centralized, structured repository designed to collect, standardize, and store data from multiple healthcare sources—EHRs, EMRs, lab databases, claims systems, workforce records, and public health registries. Unlike operational databases optimized for day-to-day transactions or clinical data repositories that serve near real-time patient views at the point of care, a data warehouse is purpose-built for analytics, quality improvement, research, and decision support.
Where It Fits in Practice
The warehouse sits downstream from raw data capture—EHRs, billing systems, lab instruments—and upstream from analytics dashboards or decision-support tools. It is the organized layer that makes analysis trustworthy and repeatable. Without it, care teams and administrators pull fragmented reports from disconnected systems, reconcile conflicting numbers by hand, and act on incomplete information.
Who Uses the Data and How
Clinicians, administrators, policymakers, and workforce planners each rely on the warehouse differently—but all depend on the same underlying data quality. In rural settings specifically, that means tracking provider-to-population ratios, modeling retention incentive scenarios, and comparing county-level MD and NP/PA supply over time. Platforms like HealthFront Baseline™ apply this infrastructure specifically to rural HCP workforce data, giving state-level programs a structured starting point without building custom pipelines from scratch.
Key Benefits of Healthcare Data Warehouse Solutions
The advantages below are tied to measurable outcomes that healthcare organizations track daily: time-to-decision, cost efficiency, quality scores, compliance posture, and workforce stability.
Consolidated Data Access for Faster, More Accurate Clinical Decisions
Fragmented data—spread across EHRs, lab systems, pharmacy records, and billing—forces care teams to make decisions with incomplete context. A data warehouse resolves this by creating a single source of structured, verified truth.
Data from disconnected systems is extracted, standardized, and made queryable in a centralized layer. Clinicians access full patient history without switching systems or waiting on manual data pulls. Instead of reconciling medication lists from three different sources, providers see one longitudinal record that flags discrepancies automatically.
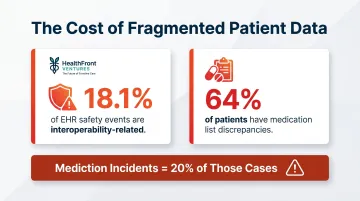
Access to complete longitudinal patient records directly reduces diagnostic errors, supports more effective treatment planning, and speeds up time-sensitive clinical decisions. Research shows that up to 18.1% of EHR-related patient safety events were interoperability-related, with medication-related incidents making up 20% of those cases. In one study, 64% of patients had medication list discrepancies, underscoring how incomplete data at the point of care increases liability exposure, misdiagnosis risk, and avoidable readmissions.
This benefit tracks against several operational KPIs:
- Time-to-diagnosis and EHR query response time
- Readmission rates and medication error rates
- Care plan accuracy
It is most pronounced in high-volume or multi-site organizations, emergency settings, and rural facilities — where care teams are smaller and cannot afford delays caused by manual data reconciliation. For rural health programs managing those constraints, workforce data adds another layer of strategic value.
Workforce Intelligence for Provider Retention and Recruitment Planning
Healthcare data warehouses are not limited to patient data. They can integrate HCP workforce data—provider tenure, compensation benchmarks, rural county staffing ratios, NP/PA utilization metrics—to support strategic workforce decisions.
By consolidating workforce data alongside patient volume and outcome data, administrators and program planners can identify retention risk factors, model staffing scenarios, and track the performance of recruitment incentives over time. For example, a state rural health office might cross-reference provider turnover rates with county-level HPSA designations and utilization patterns to identify high-risk vacancies before they occur.
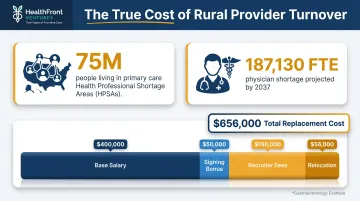
Rural healthcare organizations face severe provider shortages. Approximately 75 million people live in primary care Health Professional Shortage Areas, with a projected physician shortage of 187,130 FTE by 2037—greater shortfalls expected in nonmetro areas. Without structured workforce data, retention and recruitment decisions are made reactively rather than proactively.
Losing a primary care provider in a rural county affects thousands of patients and incurs significant replacement costs. One analysis shows that replacing a single specialist can exceed $500,000 in direct and incentive costs. A gastroenterology example totals $656,000 when base salary, signing bonus, recruiter fees, and relocation are included.
Workforce intelligence tracks against these planning metrics:
- Provider turnover rate and time-to-fill vacancies
- NP/PA utilization rates
- Staffing cost per patient visit and retention incentive ROI
This capability is most critical for rural health transformation programs, federally qualified health centers, and state-level workforce planning bodies that need quantitative baseline metrics to allocate resources and track intervention effectiveness. When workforce data is in place, those same organizations can extend the warehouse's value into population-level analytics.
Predictive Analytics and Population Health Management
A data warehouse, by centralizing multi-source historical data, creates the foundation for predictive modeling. Organizations can use it to anticipate patient risk, forecast service demand, and intervene earlier in chronic disease progression.
Standardized, longitudinal datasets allow analytics teams to run population-level analyses, train risk stratification models, and identify trends that would be invisible in isolated system data. For instance, combining EHR lab results with claims utilization data can surface patients at high risk for diabetic complications who have missed recent screenings.
Predictive analytics shifts organizations from reactive care delivery to proactive intervention, which is particularly valuable for managing high-burden conditions like diabetes, hypertension, and COPD. Diabetes prevalence is 14.3% in rural areas versus 11.2% in urban areas, and COPD mortality rates are consistently higher in rural communities.
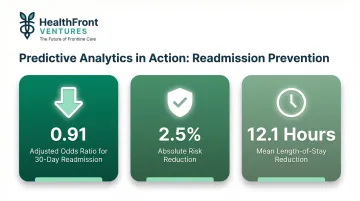
Earlier intervention reduces expensive acute care utilization, including ED visits and avoidable hospitalizations. One study of a hospital readmission prevention program targeted with predictive analytics found an adjusted odds ratio of 0.91 for 30-day readmission, an absolute risk reduction of 2.5%, and a mean length of stay reduction of 12.1 hours.
Performance tracked against this capability includes:
- Risk stratification accuracy and preventable ED visits
- Chronic condition management scores
- Cost per member per month
- Population health outcome benchmarks against value-based care contracts
This advantage scales with data volume and longitudinal depth, making it most impactful for organizations managing state health programs or population health initiatives where outcome-based performance is financially tied.
High-Value Use Cases for Healthcare Data Warehousing
The use cases below represent the most common and measurable applications of healthcare data warehouses across clinical, operational, and strategic functions.
Use Case 1: Chronic Disease and Care Gap Management
Data warehouses enable care teams to identify patients overdue for screenings, flag disease progression risks, and support coordinated management of conditions like diabetes, hypertension, and heart disease by linking lab results, visit history, and medication adherence data across systems.
How it works in practice:
A warehouse aggregates lab values (HbA1c, LDL, blood pressure), visit dates, prescription fills, and payer claims to generate automated lists of patients who fall outside quality measure thresholds. Care coordinators can prioritize outreach based on risk scores, closing care gaps before they escalate into costly complications.
The gap is sharpest in rural areas, where structural barriers already limit access to chronic disease management. Only 30.1% of rural counties have diabetes self-management education and support programs, compared to 59.6% of urban counties.
Use Case 2: Rural Workforce Planning and HCP Retention Tracking
State-level rural health programs and rural healthcare organizations use workforce data warehouses to track provider headcount by county, monitor retention incentive outcomes, model NP/PA scope-of-practice expansion impact, and establish baseline metrics for grant reporting and program evaluation.
A typical workflow:
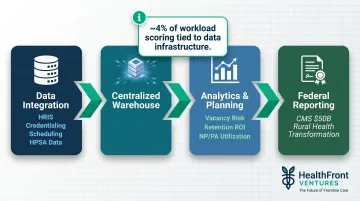
A state rural health office integrates HRIS data, credentialing records, scheduling utilization, and HPSA designation data into a centralized warehouse. Planners can then:
- Identify counties with rising vacancy risk before positions go unfilled
- Quantify the impact of retention bonuses on provider tenure
- Report standardized metrics to federal funders with audit-ready documentation
Federal funding makes this capability increasingly consequential. CMS announced $50 billion in awards under the Rural Health Transformation Program, with all 50 states participating and first-year awards averaging $200 million. Roughly 4% of workload scoring is tied to data infrastructure plans, making warehouse capabilities a measurable competitive advantage in grant applications.
Use Case 3: Operational Efficiency and Resource Allocation
Administrators use warehouse data to analyze throughput, staffing utilization, scheduling gaps, and cost drivers—driving informed decisions about capacity planning, service line investment, and operational restructuring.
How it works in practice:
By linking scheduling data, patient volume, billing records, and staffing cost data, organizations can identify underutilized clinic hours, peak demand periods, and service lines with low margin or high cost-per-visit. This visibility supports decisions like expanding urgent care hours, shifting staff between departments, or discontinuing low-value services.
Use Case 4: Regulatory Reporting and Quality Improvement
A structured data warehouse simplifies compliance by maintaining audit-ready, standardized datasets for HIPAA reporting, CMS quality measures, HEDIS metrics, and state health program performance benchmarks—reducing manual reporting burden and improving accuracy.
Example workflow:
Instead of manually abstracting charts for quarterly quality reporting, organizations map each CMS and HEDIS measure definition to a governed semantic layer in the warehouse. Automated extracts pull the required numerators and denominators, shorten submission cycles, and reduce errors.
The compliance cost burden makes this automation financially significant. Hospitals and post-acute care providers spend approximately $39 billion per year on federal regulatory compliance, covering 629 discrete requirements. Physician practices alone spend more than $15.4 billion annually reporting quality measures.
What Happens When Healthcare Data Infrastructure Is Missing or Ignored
Operating without a data warehouse means clinical and administrative teams work from fragmented systems, pulling manual reports, reconciling conflicting numbers, and making high-stakes decisions based on partial information.
Consequences compound over time:
- Quality reporting breaks down when data is inconsistent across systems. Organizations cannot verify measure performance, which leads to failed audits and missed value-based contract incentives.
- Workforce planning becomes reactive rather than strategic, driving higher turnover, longer vacancy periods, and care continuity gaps — especially damaging in rural settings where provider supply is constrained and replacement costs are high.
- Cost drivers go undetected without centralized visibility. Duplicated efforts, avoidable utilization, and inefficient resource allocation accumulate quietly because administrators have no system to surface or prioritize them.

Beyond daily operations, missing data infrastructure carries strategic consequences. Organizations without a warehouse struggle to qualify for grant funding, compete for value-based care contracts, or produce the outcome reports that state and federal stakeholders require. When funding decisions hinge on quantitative data, organizations that can't measure what they do simply can't compete for what they need.
How to Get the Most Value from a Healthcare Data Warehouse
A data warehouse delivers compounding returns when it is consistently maintained, regularly reviewed, and actively connected to organizational decision-making—not treated as a reporting archive.
Three operating conditions determine how much value you extract:
- Broad source coverage with clean ingestion: Pull from all relevant systems—EHR, workforce, claims, labs—and apply standardization and validation at the point of ingestion. Establish data quality rules, monitor exceptions, and assign clear accountability for source system accuracy.
- Governed access across functions: Define data stewardship responsibilities, role-based access controls, and change management protocols so the warehouse stays accurate and HIPAA-compliant across clinical, administrative, and leadership teams.
- Outsourced infrastructure for leaner organizations: Rural and resource-constrained organizations can skip the custom build entirely. Platforms like HealthFront Ventures' AI-Native HCP Workforce Data Warehouses deliver full data infrastructure without requiring an in-house engineering team, cutting setup time and ongoing maintenance costs.
Conclusion
A healthcare data warehouse earns its value through what it makes possible: faster clinical decisions, sharper workforce retention intelligence, and predictive analytics that improve before a crisis hits. Those advantages build on each other over time — but only when the underlying infrastructure is actively governed and consistently used.
For rural healthcare organizations in particular, this distinction matters. Data warehousing is an ongoing operational practice that requires consistent governance — not a project that ends at deployment. Organizations that build it into daily operations can track workforce trends before they become vacancies, meet reporting requirements without scrambling, and make the kind of evidence-based decisions that keep rural providers in the communities they serve.
Frequently Asked Questions
What is a healthcare data warehouse and how does it work?
A healthcare data warehouse is a centralized repository that aggregates data from EHRs, claims, labs, and other sources, standardizes it across systems, and makes it available for analysis. It serves as the organized layer between raw data capture and actionable reporting, enabling consistent, trustworthy decision-making.
How is a healthcare data warehouse different from an EHR?
An EHR captures individual patient data at the point of care—optimized for clinical transactions, not analysis. A data warehouse pulls from multiple EHRs and other systems, normalizes the data, and enables population-level reporting and strategic planning that no single EHR can support.
What are the biggest challenges in building a healthcare data warehouse?
The three most common barriers are data integration complexity across disparate systems, ensuring data quality and consistency after aggregation, and maintaining HIPAA-compliant security and governance. Outsourced solutions can reduce the infrastructure burden for smaller organizations by handling these technical challenges as a managed service.
How can rural healthcare organizations benefit from data warehousing?
Rural organizations gain workforce data visibility for provider retention and recruitment planning, population health management for high-burden chronic conditions like diabetes and COPD, and simplified compliance reporting—all without requiring large internal IT teams if using an outsourced model like HealthFront Baseline™.
What data sources does a healthcare data warehouse typically integrate?
Common sources include EHRs, claims and billing systems, lab information systems, pharmacy records, workforce and HR data, and public health registries. The broader the integration, the richer and more reliable the analysis—single-source warehouses leave critical gaps.
How do AI-native healthcare data warehouses differ from traditional ones?
AI-native warehouses embed machine learning directly into data ingestion, quality monitoring, and analytics—enabling anomaly detection and predictive modeling without manual intervention. With 86% of health systems now leveraging AI yet 72% citing data privacy concerns, governance-by-design at the warehouse layer is no longer optional.